Review Article Botulinum toxin in Recurrent Postoperative HerniasSinou Natalia 1,2, Sinou Nikoleta 1,2 , Filippou Dimitris 1,21 Medical School, National and Kapodistrian University of Athens,
2 Research and Education Institute of Biomedical Science
Corresponding Address: Natalia Sinou, sinou.natalia@gmail.comKeywords: botulinom toxin, postoperative hernias, recurrent hernias
Abstract
Incisional hernias constitute a complex issue in the field of general surgery. The traditional invasive techniques of the hernias repairing are partially efficient as
there are many recurrences. The further operations lead to numerous problems such as contamination, morbidity and damaging the tissues. A very promising method to overcome the
problems mentioned above was the introduction of the usage of Botulinum toxin A in the treatment of recurrent hernias.
Aim of the present systematic review is to evaluate the possible application of the Botulinum toxin type A before surgery and the disadvantages of this method. Detailed research
was conducted via the PubMed database using the keywords: “Recurrent” AND “Postoperative” AND “Hernias” AND “Botulinum toxin”. No further filters were applied.
The existing experience suggests that Botulinum toxin A supports the uneventful postoperative recovery after hernia surgery offering decreased tension to suture line tension
without perturbing the structure and physiology of the abdominal wall. However, it has been spontaneously associated with minor complications mainly from the respiratory
system.
Introduction
Open abdominal surgeries can lead to various complications, with ventral hernias being one of the most prevalent. Roughly 30% of patients may be affected by these hernias,
which can negatively impact their quality of life both aesthetically and due to issues like abdominal compartment syndrome.[1] The likelihood of ventral hernia occurrence increases
in patients with risk factors, such as obesity, diabetes, smoking, malignancy, infection, emergency intervention, use of steroids and immunomodulatory factors, or a
previous laparotomy.[2]
Managing incisional hernias presents a complex challenge in the field of surgery. Traditional invasive techniques, like abdominal wall reconstruction and hernia repair, offer only
partial effectiveness and can result in numerous recurrences. Repairing recurrent hernias through repeated operations carries the risk of damaging and thickening tissue even further.
Additionally, in more complicated cases of hernias requiring bridging, there are concerns about recurrence, contamination, and morbidity [3]. The component separation approach is
often considered the gold standard for certain types of hernias, while the Rives-Stoppa retromuscular technique is preferred for others because they allow for tension-free closure
and preservation of abdominal physiology. However, even these techniques do not guarantee success, as recurrence, contamination, and surgical complications remain potential risks.
Other methods like myocutaneous fascial speculums and pneumoperitonisation have proved ineffective in expanding the abdominal wall.
The primary cause of ventral hernias is often the anti-diametric movement of abdominal muscles. However, a promising alternative to surgical intervention is the non-surgical approach
known as Botox based technique. This innovative technique leverages botulinum toxin type A, produced by the clostridium botulinum, to reduce the tension exerted by these muscles,
inducing temporary paralysis that addresses the underlying cause.[4] This technique is particularly effective for large incisional hernias and those that have lost domain.[5] Aim
of the present systematic review is to evaluate the possible use of botulinum toxin type A preoperatively as well as to present the advantages and the disadvantages of this technique.
Materials and methods
Thorough research was conducted by using the PubMed database's published bibliography. The search was conducted using keywords such as "Recurrent", "Postoperative", "Hernias",
and "Botulinum toxin". Relevant data was extracted using a standard data elicitation form and following PRISMA-ScR guidelines. Out of the 34 records identified through the initial
PubMed search, no additional ones were found through references review as they were similar to the initial ones. Furthermore, 24 full-text articles were assessed for eligibility and
out of these, 10 were excluded due to non-relevant title and abstract. All 24 references assessed for eligibility were deemed relevant and fulfilled the above mentioned criteria, and
hence were used in this study.
Figure 1. Botulinum toxin in Recurrent Postoperative Hernias - PRISMA
Discussion
Botulinum toxin type A, or BTA, possesses a broad range of medical applications, including the treatment of strabismus, muscular pain, dystonia syndromes,
esophagus achalasia, hyperhidrosis, and aesthetic procedures [2]. This clostridium botulinum-derived substance works by inhibiting the release of acetylcholine from the neuromuscular
junction, resulting in muscle paralysis and elongation. Its effects become evident within 2-3 days and peak within 2 weeks, with a duration of up to 6 months that declines gradually.
Infusing the toxin into the abdominal wall muscles produces a relaxed state that tightens and repairs a hernia without resorting to invasive component separation. This approach preserves
the abdominal wall's physiology and myofascial structures [6]. As it is described in an interesting report the toxin is injected in an outpatient setting approximately four weeks before
the impending operation. [7] Under high-resolution ultrasound, five specific points are identified in patients who are positioned laterally. Two of these points are located between the
upper iliac crest and rib margin in the mid-axillary line, while the remaining three points are situated between the anterior axillary line and midclavicular line, between the costal
margin and superior iliac crest. The procedure is performed bilaterally, and each point is injected with 5ml of a solution containing 500 units of BTA dissolved in 50ml of 0.9% saline s
solution. This chemical technique results in paralysis that lasts up to four-six months and begins approximately two weeks after injection.
The diminished tension caused by the BTA enables efficient repair. However, as there is no clinical effect in the first 48 hours, the use of negative pressure ligatures
is recommended to prevent abdominal wall contraction [8].
More invasive techniques can be safely applied with guaranteed permanent results once the toxin's effects are visible, as confirmed by CT scans. The muscle did not swell during the
preoperative BTA application, as stated in the first report [9]. Another advantage of BTA lies in the flaccid paralysis of the lateral abdominal muscles, allowing the closure of large
hernias without excessive tension, reducing the likelihood of ventilation duration or postoperative complications such as abdominal hypertension and respiratory disorders [10].
BTA is preferred over invasive procedures for patients with spastic muscles disorders [8]. Additionally, BTA can be used as complementary treatment to progressive preoperative
pneumoperitoneum (PPP) when it is insufficient [11]. Lastly, BTA can also be employed postoperatively to alleviate pain.
Disadvantages. Despite its widespread use for medical purposes, the botulinum toxin A has several drawbacks that prevent its broad application. High cost is a major
barrier to access, with some insurance companies declining coverage for the repair of large ventral hernias. Moreover, some patients have reported temporary concerns, such as weakened
breath, sneezing, and coughing, due to the flaccidity of the abdominal muscle wall.[14,15} Furthermore, some patients experienced a feeling of fullness and bloating after the onset of
BTA action, with others reporting pain, bruising, and detention sensations following toxin injection.[13,16,19] Multiple reports confirm that the normal functioning of the abdominal
muscles involves contraction, aiding movement and stabilizing the spine and torso. However, the use of BTA can hinder these muscles, causing back pain through invasive
component separation and chemical paralysis. Additionally, the BTA can relax the lateral abdominal wall muscles, leading to altered respiratory physiology and
resulting in dyspnea. [13,17,18,20].
Animal experiments support the claim that BTA inhibits pain, signal, and perception transmitters beyond blocking acetylcholine secretion. [2,7]. Patients who are
hemodynamically stable [8] and non-smokers, during the application period, are the only eligible candidates for BTA treatment. Moreover, the weight loss of obese patients is a
prerequisite for BTA therapy.
However, BTA is known to cause anaphylaxis due to its constituents and exacerbate Myasthenia Gravis, making it an absolute contraindication [6]. Lastly, patients who undergo BTA must
undergo long-term follow-up to mitigate any potential side effects. [10,15].
Botulinum toxin type A is an effective and safe technique that is easily tolerated and has reversible effects without permanent complications. Separating the chemical components with BTA
allows for closure without tension, without disrupting the abdominal wall's structure or physiology. Previously thought unmanageable hernias can now be cured using this technique,
thanks to BTA's ability to induce relaxation and elongation. This eliminates the need for surgical expansion of the abdominal cavity and reduces pain and muscle tension
in the postoperative period. However, BTA may cause inconvenience to patients such as temporary concerns, weak breathing, coughing, bloating, pain, and difficulty breathing. BTA
should only be used in hematologically stable patients who do not smoke or are not obese.[21-24].
Conclusion
The healing process is safeguarded for a considerable duration due to the effects of Botox. Additionally, the utilization of Botox obstructs the occurrence of
postoperative issues including necrosis, fibrosis, recurrency, and morbidity. Despite being a relatively new approach, thorough monitoring and observation are imperative before
any conclusions about potential complications can be determined.
References
1. Deerenberg EB, Shao JM, Elhage SA, Lopez R, Ayuso SA, Augenstein VA, Heniford BT. Preoperative botulinum toxin A injection in complex abdominal wall reconstruction - a
propensity-scored matched study. Am J Surg. 2021 Sep;222(3):638-642. doi: 10.1016/j.amjsurg.2021.01.010.
2. Elstner KE, Jacombs AS, Read JW, Rodriguez O, Edye M, Cosman PH, Dardano AN, Zea A, Boesel T, Mikami DJ, Craft C, Ibrahim N. Laparoscopic repair of complex ventral
hernia facilitated by pre-operative chemical component relaxation using Botulinum Toxin A. Hernia. 2016 Apr;20(2):209-19. doi: 10.1007/s10029-016-1478-6.
3. Deerenberg EB, Elhage SA, Shao JM, Lopez R, Raible RJ, Kercher KW, Colavita PD, Augenstein VA, Heniford BT. The Effects of Preoperative Botulinum Toxin A
Injection on Abdominal Wall Reconstruction. J Surg Res. 2021 Apr;260:251-258. doi: 10.1016/j.jss.2020.10.028.
4. Bueno-Lledó J, Martinez-Hoed J, Torregrosa-Gallud A, Menéndez-Jiménez M, Pous-Serrano S. Botulinum toxin to avoid component separation in midline large hernias.
Surgery. 2020 Sep;168(3):543-549. doi: 10.1016/j.surg.2020.04.050.
5. Rodriguez-Acevedo O, Elstner KE, Jacombs ASW, Read JW, Martins RT, Arduini F, Wehrhahm M, Craft C, Cosman PH, Dardano AN, Ibrahim N. Preoperative Botulinum toxin
A enabling defect closure and laparoscopic repair of complex ventral hernia. Surg Endosc. 2018 Feb;32(2):831-839. doi: 10.1007/s00464-017-5750-3.
6. Mourad AP, De Robles MS, Winn RD. Low-Dose Pre-Operative Botulinum Toxin A Effectively Facilitates Complex Ventral Hernia Repair: A Case Report and Review of
the Literature. Medicina (Kaunas). 2020 Dec 28;57(1):14. doi: 10.3390/medicina57010014.
7. Bueno-Lledó J, Torregrosa A, Jiménez R, Pastor PG. Preoperative combination of progressive pneumoperitoneum and botulinum toxin type A in patients with loss of
domain hernia. Surg Endosc. 2018 Aug;32(8):3599-3608. doi: 10.1007/s00464-018-6089-0.
8. Ibarra-Hurtado TR, Nuño-Guzmán CM, Miranda-Díaz AG, Troyo-Sanromán R, Navarro-Ibarra R, Bravo-Cuéllar L. Effect of botulinum toxin type A in lateral abdominal
wall muscles thickness and length of patients with midline incisional hernia secondary to open abdomen management. Hernia. 2014 Oct;18(5):647-52. doi: 10.1007/s10029-014-1280-2.
9. Ibarra-Hurtado TR, Nuño-Guzmán CM, Echeagaray-Herrera JE, Robles-Vélez E, de Jesús González-Jaime J. Use of botulinum toxin type a before abdominal wall
hernia reconstruction. World J Surg. 2009 Dec;33(12):2553-6. doi: 10.1007/s00268-009-0203-3.
10. Elstner KE, Read JW, Rodriguez-Acevedo O, Cosman PH, Dardano AN, Jacombs AS, Edye M, Zea A, Boesel T, Mikami DJ, Ibrahim N. Preoperative chemical component
relaxation using Botulinum toxin A: enabling laparoscopic repair of complex ventral hernia. Surg Endosc. 2017 Feb;31(2):761-768. doi: 10.1007/s00464-016-5030-7.
11. Tashkandi A, Bueno-Lledó J, Durtette-Guzylack J, Cayeux A, Bukhari R, Rhaeim R, Malinovski JM, Kianmanesh R, Renard Y. Adjunct botox to preoperative progressive
pneumoperitoneum for incisional hernia with loss of domain: no additional effect but may improve outcomes. Hernia. 2021 Dec;25(6):1507-1517. doi: 10.1007/s10029-021-02387-8.
12. Soltanizadeh S, Helgstrand F, Jorgensen LN. Botulinum Toxin A as an Adjunct to Abdominal Wall Reconstruction for Incisional Hernia. Plast Reconstr Surg Glob Open.
2017 Jun 21;5(6):e1358. doi: 10.1097/GOX.0000000000001358.
13. Farooque F, Jacombs AS, Roussos E, Read JW, Dardano AN, Edye M, Ibrahim N. Preoperative abdominal muscle elongation with botulinum toxin A for complex incisional
ventral hernia repair. ANZ J Surg. 2016 Jan-Feb;86(1-2):79-83. doi: 10.1111/ans.13258.
14. van Rooijen MMJ, Yurtkap Y, Allaeys M, Ibrahim N, Berrevoet F, Lange JF. Fascial closure in giant ventral hernias after preoperative botulinum toxin a and
progressive pneumoperitoneum: A systematic review and meta-analysis. Surgery. 2021 Sep;170(3):769-776. doi: 10.1016/j.surg.2021.03.027.
15. Elstner KE, Read JW, Saunders J, Cosman PH, Rodriguez-Acevedo O, Jacombs ASW, Martins RT, Ibrahim N. Selective muscle botulinum toxin A component paralysis in
complex ventral hernia repair. Hernia. 2020 Apr;24(2):287-293. doi: 10.1007/s10029-019-01939-3.
16. Seretis F, Chrysikos D, Samolis A, Troupis T. Botulinum Toxin in the Surgical Treatment of Complex Abdominal Hernias: A Surgical Anatomy Approach, Current Evidence
and Outcomes. In Vivo. 2021 Jul-Aug;35(4):1913-1920. doi: 10.21873/invivo.12457.
17. Yurtkap Y, van Rooijen MMJ, Roels S, Bosmans JML, Uyttebroek O, Lange JF, Berrevoet F. Implementing preoperative Botulinum toxin A and progressive pneumoperitoneum
through the use of an algorithm in giant ventral hernia repair. Hernia. 2021 Apr;25(2):389-398. doi: 10.1007/s10029-020-02226-2.
18. Elstner KE, Read JW, Rodriguez-Acevedo O, Ho-Shon K, Magnussen J, Ibrahim N. Preoperative progressive pneumoperitoneum complementing chemical component relaxation
in complex ventral hernia repair. Surg Endosc. 2017 Apr;31(4):1914-1922. doi: 10.1007/s00464-016-5194-1.
19. Bueno-Lledó J, Torregrosa A, Ballester N, Carreño O, Carbonell F, Pastor PG, Pamies J, Cortés V, Bonafé S, Iserte J. Preoperative progressive pneumoperitoneum and
botulinum toxin type A in patients with large incisional hernia. Hernia. 2017 Apr;21(2):233-243. doi: 10.1007/s10029-017-1582-2.
20. Catalán-Garza V, Peña-Soria MJ, Sáez-Carlin P, Cabeza-Gómez JJ, García-Fernández A, Torres-García AJ. Long-term results of botulinum toxin type A in complex abdominal
wall repair and review of the literature. Updates Surg. 2020 Dec;72(4):1201-1206. doi: 10.1007/s13304-020-00775-w.
21. Bueno-Lledó J, Carreño-Saenz O, Torregrosa-Gallud A, Pous-Serrano S. Preoperative Botulinum Toxin and Progressive Pneumoperitoneum in Loss of Domain Hernias-Our First
100 Cases. Front Surg. 2020 Feb 28;7:3. doi: 10.3389/fsurg.2020.00003.
22. Weissler JM, Lanni MA, Tecce MG, Carney MJ, Shubinets V, Fischer JP. Chemical component separation: a systematic review and meta-analysis of botulinum toxin for
management of ventral hernia. J Plast Surg Hand Surg. 2017 Oct;51(5):366-374. doi: 10.1080/2000656X.2017.1285783.
23. Tang FX, Zong Z, Xu JB, Ma N, Zhou TC, Chen S. Combination of Preoperative Progressive Pneumoperitoneum and Botulinum Toxin A Enables the Laparoscopic Transabdominal
Preperitoneal Approach for Repairing Giant Inguinoscrotal Hernias. J Laparoendosc Adv Surg Tech A. 2020 Mar;30(3):260-266. doi: 10.1089/lap.2019.0669.
24. Tang FX, Ma N, Huang E, Ma T, Liu CX, Chen S, Zong Z, Zhou TC. Botulinum Toxin A Facilitated Laparoscopic Repair of Complex Ventral Hernia. Front Surg. 2022
Jan 10;8:803023. doi: 10.3389/fsurg.2021.803023.
Χρησιμοποιούμε cookies για να σας προσφέρουμε την καλύτερη δυνατή εμπειρία στη σελίδα μας. Εάν συνεχίσετε να χρησιμοποιείτε τη σελίδα, θα υποθέσουμε πως είστε ικανοποιημένοι με αυτό..
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.
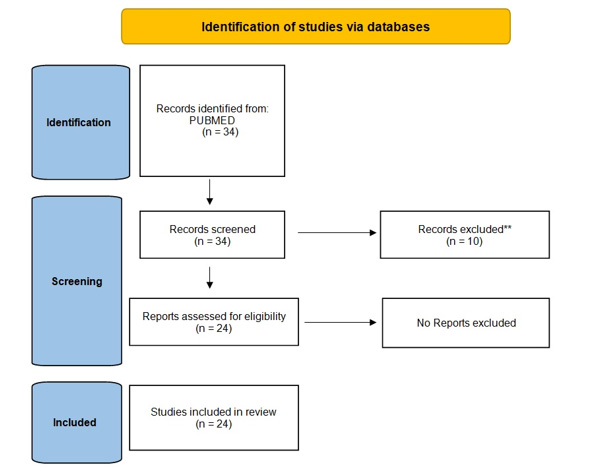 Figure 1. Botulinum toxin in Recurrent Postoperative Hernias - PRISMA
Figure 1. Botulinum toxin in Recurrent Postoperative Hernias - PRISMA