Case Report Thyroidea-Ima Artery: Α case report Sampsakos-Mariolis Theodoros1,2 Sinou Nikoleta3,4 Metheniti Panagiota1,2 Koumenis Andreas1,2 Sinou Natalia3,4 Filippou Dimitrios3,5
1 Department of Anatomy-Histology and Embryology, Nursing School, National and Kapodestrian University of Athens, Greece
2 Department of Surgery, Nursing School, Agii Anargiri Anticancer Hospital, Athens, Greece
3 Research and Education Institute in Biomedical Sciences, Pireaus, Greece
4 Medical School, National and Kapodestrian University of Athens, Athens, Greece
5 Department of Anatomy, Medical School, National and Kapodestrian University of Athens, Greece
Abstract
Thyroidea ima artery is a rare anatomical entity that may present in 3-10% of the general population as an embryonic remaining. It is an accessory vesicle for the blood
supply thyroid’s gland isthmus and lower lobe. The artery may also supply the trachea and the parathyroid gland. The artery may origin from the brachiocephalic trunk, the arch of
aorta or even from the left common carotid artery. The knowledge of this vascular anatomic anomaly is important for tracheal, thyroid and parathyroid surgeries. We present a rare
case of a thyroidea-ima artery (TIA) that was discovered during thyroid surgery.
Correspondence Address: Nikoleta Sinou, nikoletta.sinou@gmail.com
Introduction
An extend part of the thyroid gland (TG), the inferior part and the isthmus, is supplied from the inferior thyroid artery (ITA). The upper part (36%) of the gland is
supplied from the superior thyroid artery (STA). Occasionally, a small auxiliary artery is present and provides with blood the thymus gland, the thyroid gland and the parathyroid
glands. This artery is called as Thyroid IMA Artery (TIA), or lowest thyroid artery. The artery first described from Neubauer in 1772 as an artery that marches along the anterior
surface of trachea and can also been found as Neubauer artery. The origin of TIA varies from the brachiocephalic artery 74%, the aortic arch 7.7%, the left common carotid artery 1.9%,
the left internal thoracic artery 1.9%, the right common carotid artery 9.6%, the right internal thoracic artery 4.8%, the subclavian artery and the vertebral artery. TIA provides with
blood the isthmus and the inferior poles of the thyroid gland and may follow various courses. It is also usual for TIA to coexist with a brachiocephalic-carotid trunk, a devious right
subclavian artery of retroesophageal course, a variable march of the inferior laryngeal nerve (non-recurrent and recurrent) and the bilateral absence of the inferior thyroid artery.
It is high yield for surgeons to have awareness of the IMA and its variabilities in order to avoid massive intraoperative hemorrhages during tracheotomy and cricothyroidotomy.
We present a rare case of thyroid IMA artery that was identified during a thyroidectomy performed to a male patient.
Case report
A 59-year-old Caucasian male underwent total thyroidectomy for thyroid cancer. He had not undergone any other previous surgeries in the thyroid gland.During the operation,
the TIA was found arising from left common carotid artery (Figure 1). The superior and inferior thyroid artery and vein recognized, ligated and dissected. During the dissection of the
tissues above trachea we found thyroid IMA over the trachea entering the inferior surface of the gland in the region of isthmus. This is carefully separated from the trachea with a
blunt- nosed hemostat and ligated in the usual fashion.
Figure 1: The thyroidea-ima artery, during thyroidectomy.
We routinely dissect and expose the common carotid artery before mobilizing the thyroid gland (lateral to medial approach). By this approach, a good vascular control is achieved and
inadvertent injury to blood vessels is avoided even if the thyroid gland is large and extending retrosternal. The three structures of significance between common carotid and trachea
are the recurrent laryngeal nerve, inferior thyroid artery and middle thyroid vein. Any anomalous vessel in this location can be easily identified and dissected to its origin thereby
avoiding injury.
In the present case TIA was found arising from the left common carotid artery and it was dissected and ligated carefully, without injuring it and avowing any possible bleeding.
Discussion
Embryologically, the thyroid gland has a rich vascular supply, as it consists one of the most important endocrine glands in the human body. The main arteries that supply blood
to the thyroid gland are the superior thyroid artery, inferior thyroid artery, and sometimes the thyroid Ima artery (1). Specifically, superior thyroid artery is typically the first
branch of the external carotid artery (2). It supplies blood to the upper part of the thyroid gland and gives off branches that provide blood to surrounding muscles and structures in
the neck. As regards the inferior thyroid artery arises from the thyrocervical trunk, which is a branch of the subclavian artery. This artery supplies blood to the lower part of the
thyroid gland. It usually has two branches: a superior branch and an inferior branch, both of which contribute to the blood supply of the thyroid gland. The TIA is not present in everyone,
and when it is present, it can be a variation in the blood supply of the thyroid gland. This artery is relatively small and inconsistent in its occurrence (3,4).
Developmental anatomy of IMA. The aortic arch and the thyroid gland format during the 3rd and 7rd gestational week. The thyroid gland has an extensive arterial supply, and most
of the arteries regress. The remaining arteries that supply the thyroid gland after the birth are the superior and the inferior thyroid arteries. The excessive vascularization of
the arteries may lead to the morphogenesis of the thyroid gland. Thyroid defects, cardiovascular variants and also the TIA variation occur from disruptions between thyroid gland
morphogenesis and angiogenesis (5).
The thyroid-IMA artery or Arteria thyroid-ima or thyroid artery of Neubauer, firstly described by the German Neubauer in 1772, is an anatomical anomaly that commonly functions as an
accessory blood supply for the isthmus and inferior aspect for the thyroid (6). The artery also supplies the trachea, the parathyroid gland and the thymus gland in rare cases. The IMA
artery occurs in 3-10% of the population as a persistent embryonic remaining (3).
Although thyroid-IMA arises mainly from the brachiocephalic trunk, it may also originate from the aortic arch, the right common carotid artery, the subclavian artery, the cardio phrenic
artery, the thyrocervical trunk or the internal mammary artery (7,8). The thyroid-IMA is located on the right side, crosses the trachea to the bottom of thyroid gland and its size
varies in 3-5mm in diameter (2). Some studies suggest that ethnic and anthropological factors may affect the incidence of the thyroid-IMA artery concerning people of Asia (10%),
compered to the Europeans (6%) (2,8-10). A branch of the superior thyroid arteries or the inferior artery replaces the opposite inferior thyroid artery, when it is absent (1).
Clinical significance. Due to its small size and its scarce presence, thyroidea-ima artery can easily be injured during surgical operations. Therefore, an accurate knowledge of the
vessels of the thyroid gland, of the parathyroid gland and more specific of the variations and the anomalies of their vessels, is important in order to avoid injury or fatal
hemorrhage during thyroid, parathyroid, tracheal, mediastinal surgeries and tracheostomy. However, to our knowledge, there is no specific method for surgeons in order to exclude this
possible bleeding, except for their aware of arteries variations and their careful and fine movements (6,7).
Tracheostomy is required in emerge situations where the airway is not open. It can be done either percutaneously or surgically. In the percutaneous tracheostomy, the preferred site
of entry is between the first and second or second and third tracheal rings. It is of high importance that surgeons identify the anatomical landmarks of the cricoid cartilage and
the sternal notch. The surgical tracheostomy can be done in the area between the second and third or third and forth tracheal rings. Thyroid-IMA artery mostly originates from the
right side and therefore, the endotracheal tube should be inserted on the left side of the midline. In both cases the thyroid-IMA artery can easily be injured and cause fatal
hemorrhage and only the urgent sternotomy can finally control the bleeding and save the patient’s life (7).
Therefore, on scheduled surgeries, thyroid-IMA artery is important to have been detected under ultra sound sonography. In all cases, thyroid vessels must be preserved during surgeries,
as they supply the endocrine gland (5).
Conclusion
Thyroid-IMA artery may be present with numerous variants. The ignorance of this anatomical variation may lead to massive hemorrhages during surgeries in the trachea, the thyroid
and the parathyroid glands. It is of great importance for surgeons to have an adequate knowledge of the regional anatomy and the vascular variabilities so as to avoid fatal complications.
It is also of great significance for surgeons to be prepared for the upcoming surgery with multiple scans in order to have a good awareness of the vascular anatomy of the
specific incident.
Conflicts of interest
All authors have no conflicts of interest to disclose.
Funding Policy
There is no source of funding for this research.
Ethical approval
This is a a case report for which the patient provided written informed consent. Ethical approval has also been provided by the ethical committee of the General & Anticancer
Hospital of Kifissia.
Consent Form
Written consent for the publication of this case report and accompanying images was obtained from the patient. The consent can be provided to the Editor if he asks so.
The written approval of the Ethical Committee of our Institution is also available on request.
References
1. Yilmaz E, Celik HH, Durgun B, Atasever A, Ilgi S. Arteria thyroidea ima arising from the brachiocephalic trunk with bilateral absence of inferior thyroid arteries:
a case report. Surg Radiol Anat. 1993;15(3):197-9. doi: 10.1007/BF01627705. PMID: 8235962.
2. Yohannan DG, Rajan R, Chandran AB, Krishnapillai R. An unusual origin and course of the thyroidea ima artery, with absence of inferior thyroid artery bilaterally.
Surg Radiol Anat. 2019 Feb;41(2):235-237. doi: 10.1007/s00276-018-2122-1. Epub 2018 Oct 25. PMID: 30361839.
3. "Thyroidea ima artery (anatomy)". General Practice Notebook. Retrieved 21 January 2016.
4. Natsis K, Didagelos M, Gkiouliava A, Lazaridis N, Vyzas V, Piagkou M. The aberrant right subclavian artery: cadaveric study and literature review. Surg Radiol Anat. 2017 May;
39(5):559-565. doi: 10.1007/s00276-016-1796-5. Epub 2016 Dec 20. Erratum in: Surg Radiol Anat. 2017 Sep 14; PMID: 27999944.
5. Totlis T, Natsis K, Achlatis V, Pettas T, Piagkou M. Thyroidea ima artery multiple branching pattern over the trachea. Surg Radiol Anat. 2023 Jul;45(7):813-817.
doi: 10.1007/s00276-023-03156-1. Epub 2023 Apr 27. PMID: 37106242; PMCID: PMC10317869.
6. Laphatrada Yurasakpong , Chanin Nantasenamat , Sirorat Janta , Pinthusorn Eiamratchanee , James Coey , Arada Chaiyamoon , Nutmethee Kruepunga , Thanyaporn Senarai ,
Martin Franz Langer , Krai Meemon , Athikhun Suwannakhan. The decreasing prevalence of the thyroid ima artery: A systematic review and machine learning assisted meta-analysis.
https://doi.org/10.1016/j.aanat.2021.151803
7. Kamparoudi P, Paliouras D, Gogakos AS, Rallis T, Schizas NC, Lazopoulos A, Chatzinikolaou F, Sarafis P, Serchan P, Katsikogiannis N, Sarika E, Zarogoulidis P, Karapantzos I,
Barbetakis N. Percutaneous tracheostomy-beware of the thyroidea-ima artery. Ann Transl Med. 2016 Nov;4(22):449. doi: 10.21037/atm.2016.11.04. PMID: 27999783; PMCID: PMC5159410.
8. Karacan A, Türkvatan A, Karacan K. Anatomical variations of aortic arch branching: evaluation with computed tomographic angiography. Cardiol Young.
2014 Jun;24(3):485-93. doi: 10.1017/S1047951113000656. Epub 2013 May 22. PMID: 23694814.
9. Esen K, Ozgur A, Balci Y, Tok S, Kara E. Variations in the origins of the thyroid arteries on CT angiography. Jpn J Radiol. 2018 Feb;36(2):96-102.
doi: 10.1007/s11604-017-0710-3. Epub 2017 Dec 4. PMID: 29204764.
10. Natsis K, Piagkou M, Lazaridis N, Kalamatianos T, Chytas D, Manatakis D, Anastasopoulos N, Loukas M. A systematic classification of the left-sided aortic arch
variants based on cadaveric studies' prevalence. Surg Radiol Anat. 2021 Mar;43(3):327-345. doi: 10.1007/s00276-020-02625-1. Epub 2021 Jan 2. PMID: 33386933.
Accessibility Bar
visibility_offDisable flashes
titleMark headings
settingsBackground Color
zoom_outZoom out
zoom_inZoom in
remove_circle_outlineDecrease font
add_circle_outlineIncrease font
spellcheckReadable font
brightness_highBright contrast
brightness_lowDark contrast
format_underlinedUnderline links
font_downloadMark links
Reset all optionscached
Χρησιμοποιούμε cookies για να σας προσφέρουμε την καλύτερη δυνατή εμπειρία στη σελίδα μας. Εάν συνεχίσετε να χρησιμοποιείτε τη σελίδα, θα υποθέσουμε πως είστε ικανοποιημένοι με αυτό..
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.
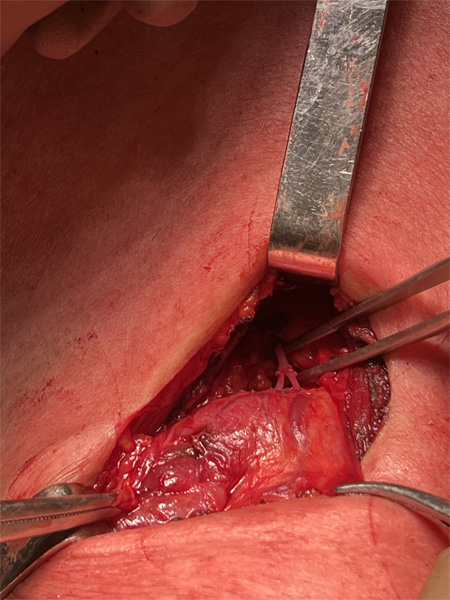 Figure 1: The thyroidea-ima artery, during thyroidectomy.
We routinely dissect and expose the common carotid artery before mobilizing the thyroid gland (lateral to medial approach). By this approach, a good vascular control is achieved and
inadvertent injury to blood vessels is avoided even if the thyroid gland is large and extending retrosternal. The three structures of significance between common carotid and trachea
are the recurrent laryngeal nerve, inferior thyroid artery and middle thyroid vein. Any anomalous vessel in this location can be easily identified and dissected to its origin thereby
avoiding injury.
In the present case TIA was found arising from the left common carotid artery and it was dissected and ligated carefully, without injuring it and avowing any possible bleeding.
Figure 1: The thyroidea-ima artery, during thyroidectomy.
We routinely dissect and expose the common carotid artery before mobilizing the thyroid gland (lateral to medial approach). By this approach, a good vascular control is achieved and
inadvertent injury to blood vessels is avoided even if the thyroid gland is large and extending retrosternal. The three structures of significance between common carotid and trachea
are the recurrent laryngeal nerve, inferior thyroid artery and middle thyroid vein. Any anomalous vessel in this location can be easily identified and dissected to its origin thereby
avoiding injury.
In the present case TIA was found arising from the left common carotid artery and it was dissected and ligated carefully, without injuring it and avowing any possible bleeding.