REVIEWGLP-1 Receptor Agonists and Cholelithiasis: A Comprehensive ReviewGiotas Ilias1, Demeneopoulou Eirini1, Filippou Dimitrios1,2
1 Medical School, National and Kapodistrian University of Athens
2 Research and Education Institute in Biomedical Sciences, Piraeus, Greece
Correspondence Address: Ilias GIOTAS, Address: Mikras Asias 75, Tax Code: 115 27, Town-Country: Athens-Greece, Email: iliasgiotas2001@gmail.com-------/iokl
Abstract
GLP-1 receptor agonists (GLP-1 RAs) have emerged as a novel class of antidiabetic medications, displaying potential in optimizing glycemic control and offering
cardiovascular advantages for individuals with type 2 diabetes. Moreover, GLP-1 receptor agonists are utilized in the treatment of childhood and adolescent obesity.
Currently, there are seven GLP-1 receptor agonists available, including exenatide twice-daily, exenatide extended-release (ER) once-weekly, lixisenatide once-daily,
liraglutide once-daily, dulaglutide once-weekly, semaglutide once-weekly, and oral semaglutide once-daily.
Aim of this systematic review is to provide an all-inclusive analysis of the existing literature exploring the association between GLP-1 receptor agonists and cholelithiasis,
assess the risk of cholelithiasis induced by GLP-1 RAs, and establish its significance. A thorough examination was conducted using the PubMed database with the keywords:
“glp-1 receptor agonists” AND “glp-1” AND “cholelithiasis.” No further filters were applied. The last research was conducted on 26 November 2023.
Based on the research findings, it has been determined that the utilization of Glp-1 RAs in the management of type 2 diabetes and obesity may be connected to a heightened
susceptibility to cholelithiasis. However, further extensive investigations are necessitated to conclusively ascertain the statistical significance of this increased risk
in relation to the use of GLP-1 RAs for obesity treatment.
Keywords: glp-1, glp-1 receptor agonists, cholelithiasis, obesity, type 2 diabetes
Introduction
GLP-1 receptor agonists exhibit insulinotropic and glucagon static properties, exhibiting considerable efficacy correlated with glucose levels. Consequently, they
effectively reduce elevated plasma glucose concentrations.(2) Since 2005, GLP-1 RAs have been approved for the treatment of type 2 diabetes and are currently recommended in
the initial stages of the treatment protocol. This recommendation is based on the proven benefits of GLP-1 RAs, which include weight reduction, glycemic efficacy, and
favorable cardiovascular and renal health outcomes, as indicated in the latest guidelines.(5) Additionally, GLP-1 receptor agonists have a central mechanism of action
that effectively decreases appetite and food consumption, making them a valuable therapeutic option for addressing obesity.(9) However, there have been reports of
gallbladder-related adverse events (such as cholelithiasis and cholecystitis) in clinical trials that study the metabolic effects of GLP-1Ras.
Materials and Methods
Detailed research was conducted through the published bibliography via PubMed database. The keywords used for the search were “medical”, “cannabis”, “in”, “cancer”
and “pain”. Data were extracted utilizing a common data elicitation form, using the aforementioned keywords. The study was made with respect to the PRISMA 2020 flow diagram for
new systematic reviews which included searches of databases, registers and other sources guidelines. Specifically, as regards the PRISMA, the records that were initially identified
through PubMed search were 124. These results derived after applying a filter of the last 5 years. There were 3 additional ones through review of references. Also, the full text
articles assessed for eligibility were 14, and the records excluded articles, title and abstract non relevant were 110. There was 1 extra suitable article derived from the similar
articles. All the reports assessed for eligibility were relevant, but 1 of them was written in german, so it was excluded. No duplicates were found. Finally, 17 references
fulfilled the above-mentioned criteria and used in the present work.
Figure 1: PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources **: title and abstract non relevant
Results
Research has shown that GLP-1 receptor agonists have been associated with an increased risk of cholelithiasis among patients. While some studies have found this risk to
be significant, others have been unable to provide definitive evidence. As a result, a clear conclusion cannot be drawn at this time. However, when considering the favorable
effects of these drugs on glucose metabolism, blood pressure, body weight, and cardiovascular and renal health, the overall risk/benefit profile of these agents for treating
type 2 diabetes and obesity patients is beneficial. It is recommended to assess the presence of gallstones and risk factors for cholelithiasis in all patients before initiating
incretin-based therapy.
Table: Data derived from the summary of product characteristics, as the manuscripts did not describe these data.
Discussion
Semaglutide, a Glp-1 RA that has undergone investigation, is being used as a subcutaneous treatment once a week at a dose of 2.4 mg in adults with obesity, in combination with lifestyle intervention.
This treatment has demonstrated clinically proven benefits in improving cardiometabolic risk factors and promoting weight loss. Out of a group of 201 participants, only five individuals (4%) in the
semaglutide group experienced acute cholelithiasis, whereas none of the 67 participants in the placebo group had a similar occurrence. However, the researchers did not consider this percentage to be statistically
significant.(1) Additionally, a separate study revealed that cholelithiasis was observed with greater frequency in the group receiving semaglutide compared to the group receiving a placebo
(0.6% versus 0.1% with placebo).(2) In the same study, findings indicated an elevated risk of cholelithiasis (2.5% versus 1.0%) among patients receiving liraglutide, a Glp-1 RA employed in the treatment
of obesity.(2) There is documented evidence of a 28% increased risk for cholelithiasis with GLP-1RA treatment. However, it remains uncertain whether this risk is consistent across all agents.(2) Recently
released data confirmed that therapy with GLP-1 receptor agonists is associated with a significantly increased risk of cholelithiasis (MH-OR [95% CI] 1.30 [1.01-1.68], P = .041).(3) Further research has
verified that the administration of GLP-1 RAs is correlated with heightened risks of cholelithiasis (RR, 1.27; 95% CI, 1.10-1.47; I2 = 0%). A detailed breakdown of these risks for each individual agent is
also provided.(4) In comparison to the control group, randomization to liraglutide and dulaglutide treatments showed an elevated risk for gallbladder or biliary diseases (RR, 1.79; 95% CI, 1.45-2.25 and
RR, 1.35; 95% CI, 1.06-1.73 respectively). Randomization to subcutaneous semaglutide and exenatide also demonstrated an increased risk, although it was not statistically significant
(RR, 1.28; 95% CI, 0.99-1.65 and RR, 1.23; 95% CI, 1.00-1.52 respectively). On the other hand, oral semaglutide, lixisenatide, and albiglutide did not exhibit an increased risk. Notably, higher doses of
subcutaneous semaglutide (≥1.0 mg) were associated with an increased incidence of gallbladder or biliary diseases (RR, 1.58; 95% CI, 1.13-2.22).(4) Moreover, the utilization of GLP-1 RAs exhibited a
substantial correlation with elevated risks of cholelithiasis at higher dosages (RR, 1.56; 95% CI, 1.36-1.78), nonetheless, no notable association was observed at lower dosages
(RR, 0.99; 95% CI, 0.74-1.33; P = .006 for interaction).(4) A lengthier period of treatment with GLP-1 RAs (greater than 26 weeks) was found to have a higher probability of increasing the risk for
gallbladder or biliary disease (relative risk (RR), 1.40; 95% confidence interval (CI), 1.26-1.56). However, a shorter duration of treatment (equal to or less than 26 weeks) did not exhibit the same
association (RR, 0.79; 95% CI, 0.48-1.31; p=0.03 for interaction).(4) Tirzepatide, a dual glucose-dependent insulinotropic peptide (GIP) and glucagon-like peptide-1 receptor agonist (GLP-1 RA), has
obtained approval from the US Food and Drug Administration in May 2022.(5) In various studies, incidents of cholelithiasis were observed, but the combined proportion was found to be statistically
insignificant at 0.95% (95% CI, 0.51%-1.52%) with the 5-mg dose.(5) Additionally, it should be noted that the incidence of cholelithiasis showed a further decrease with the administration of
both 10- and 15-mg doses, however, no statistically significant differences were found between these two doses.(5) Reports of cholelithiasis were higher with both formulations of semaglutide
(oral-subcutaneous) versus comparators, consistent with a meta-analysis that reported a significant increase in cholelithiasis with GLP-1RAs versus comparators.(6) In the context of Asian patients
with type 2 diabetes, a notable correlation between GLP-1RAs and heightened risk of cholelithiasis was observed, particularly among patients over the age of 60, female patients, and those undergoing
treatment for more than 120 days following initiation.(7) Liraglutide, but not dulaglutide, was associated with an elevated risk.(7) Moreover, calculating Mantel-Haenszel odds ratio (MH-OR, 95%CI),
GLP1-RA significantly increased the risk of cholelithiasis (MH-OR 1.28 [1.11, 1.48]).(8) Cholelithiasis was detected in 2.5% of patients who received liraglutide, compared to 1.0% of patients who
received a placebo.(9) A possible mechanism of biliary sludge and bile stone formation could be decreased gallbladder motility. Exenatide and albiglutide, based on acute intervention studies,
demonstrated a reduction in gallbladder emptying induced by cholecystokinin. Changes in bile salts, specifically altered deoxycholic acid levels in plasma following liraglutide treatment, may
lead to supersaturated bile. Nevertheless, the clinical implications of these alterations remain uncertain.(2,10)
Conclusion
The usage of GLP-1 RAs has been approved for the treatment of type 2 diabetes since 2005. In recent years, these agents have also been included in the treatment protocol for weight loss and obesity.
Due to this reason, not many studies have been done regarding to treatment of obesity with GLP-1 RAs. So, we cannot extract with assurance that the increased risk of cholelithiasis, due to these agents,
is statistically significant. It is imperative to evaluate the overall beneficial risk/benefit profile of treatment for each patient, considering their individual risk factors. This approach ensures that
treatment is tailored to each patient’s needs and that the benefits outweigh any potential risks.
References
1. Weghuber D, Barrett T, Barrientos-Pérez M, Gies I, Hesse D, Jeppesen OK, Kelly AS, Mastrandrea LD, Sørrig R, Arslanian S; STEP TEENS Investigators. Once-Weekly Semaglutide in Adolescents with Obesity. N Engl J Med. 2022 Dec 15;387(24):2245-2257. doi: 10.1056/NEJMoa2208601. Epub 2022 Nov 2. PMID: 36322838; PMCID: PMC9997064.
2. Smits MM, Van Raalte DH. Safety of Semaglutide. Front Endocrinol (Lausanne). 2021 Jul 7;12:645563. doi: 10.3389/fendo.2021.645563. Erratum in: Front Endocrinol (Lausanne). 2021 Nov 10;12:786732. PMID: 34305810; PMCID: PMC8294388.
3. Monami M, Nreu B, Scatena A, Cresci B, Andreozzi F, Sesti G, Mannucci E. Safety issues with glucagon-like peptide-1 receptor agonists (pancreatitis, pancreatic cancer and cholelithiasis): Data from randomized controlled trials. Diabetes Obes Metab. 2017 Sep;19(9):1233-1241. doi: 10.1111/dom.12926. Epub 2017 Jun 20. PMID: 28244632.
4. He L, Wang J, Ping F, Yang N, Huang J, Li Y, Xu L, Li W, Zhang H. Association of Glucagon-Like Peptide-1 Receptor Agonist Use With Risk of Gallbladder and Biliary Diseases: A Systematic Review and Meta-analysis of Randomized Clinical Trials. JAMA Intern Med. 2022 May 1;182(5):513-519. doi: 10.1001/jamainternmed.2022.0338. PMID: 35344001; PMCID: PMC8961394.
5. Mishra R, Raj R, Elshimy G, Zapata I, Kannan L, Majety P, Edem D, Correa R. Adverse Events Related to Tirzepatide. J Endocr Soc. 2023 Jan 26;7(4):bvad016. doi: 10.1210/jendso/bvad016. PMID: 36789109; PMCID: PMC9915969.
6. Aroda VR, Erhan U, Jelnes P, Meier JJ, Abildlund MT, Pratley R, Vilsbøll T, Husain M. Safety and tolerability of semaglutide across the SUSTAIN and PIONEER phase IIIa clinical trial programmes. Diabetes Obes Metab. 2023 May;25(5):1385-1397. doi: 10.1111/dom.14990. Epub 2023 Feb 21. PMID: 36700417.
7. Dong YH, Wu JH, Chang CH, Lin JW, Wu LC, Toh S. Association between glucagon-like peptide-1 receptor agonists and biliary-related diseases in patients with type 2 diabetes: A nationwide cohort study. Pharmacotherapy. 2022 Jun;42(6):483-494. doi: 10.1002/phar.2688. Epub 2022 May 17. PMID: 35508702.
8. Nreu B, Dicembrini I, Tinti F, Mannucci E, Monami M. Cholelithiasis in patients treated with Glucagon-Like Peptide-1 Receptor: An updated meta-analysis of randomized controlled trials. Diabetes Res Clin Pract. 2020 Mar;161:108087. doi: 10.1016/j.diabres.2020.108087. Epub 2020 Feb 19. PMID: 32084455.
9. Pizzimenti V, Giandalia A, Cucinotta D, Russo GT, Smits M, Cutroneo PM, Trifirò G. Incretin-based therapy and acute cholecystitis: a review of case reports and EudraVigilance spontaneous adverse drug reaction reporting database. J Clin Pharm Ther. 2016 Apr;41(2):116-8. doi: 10.1111/jcpt.12373. Epub 2016 Mar 2. PMID: 26936090.
10. Gether IM, Nexøe-Larsen C, Knop FK. New Avenues in the Regulation of Gallbladder Motility-Implications for the Use of Glucagon-Like Peptide-Derived Drugs. J Clin Endocrinol Metab. 2019 Jul 1;104(7):2463-2472. doi: 10.1210/jc.2018-01008. PMID: 30137354.
Accessibility Bar
visibility_offDisable flashes
titleMark headings
settingsBackground Color
zoom_outZoom out
zoom_inZoom in
remove_circle_outlineDecrease font
add_circle_outlineIncrease font
spellcheckReadable font
brightness_highBright contrast
brightness_lowDark contrast
format_underlinedUnderline links
font_downloadMark links
Reset all optionscached
Χρησιμοποιούμε cookies για να σας προσφέρουμε την καλύτερη δυνατή εμπειρία στη σελίδα μας. Εάν συνεχίσετε να χρησιμοποιείτε τη σελίδα, θα υποθέσουμε πως είστε ικανοποιημένοι με αυτό..
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.
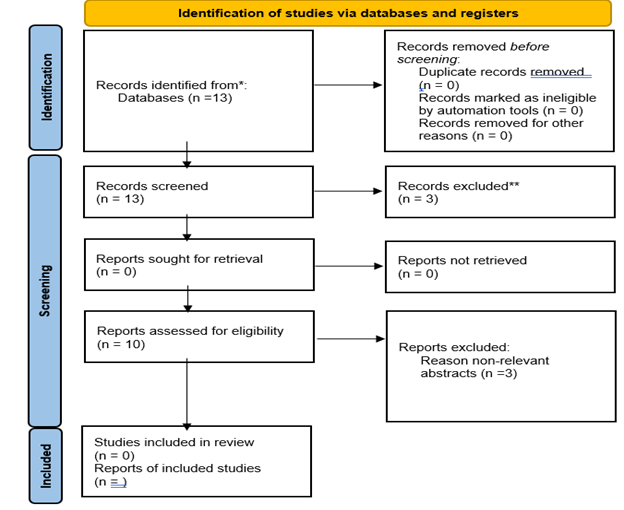 Figure 1: PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources **: title and abstract non relevant
Figure 1: PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources **: title and abstract non relevant
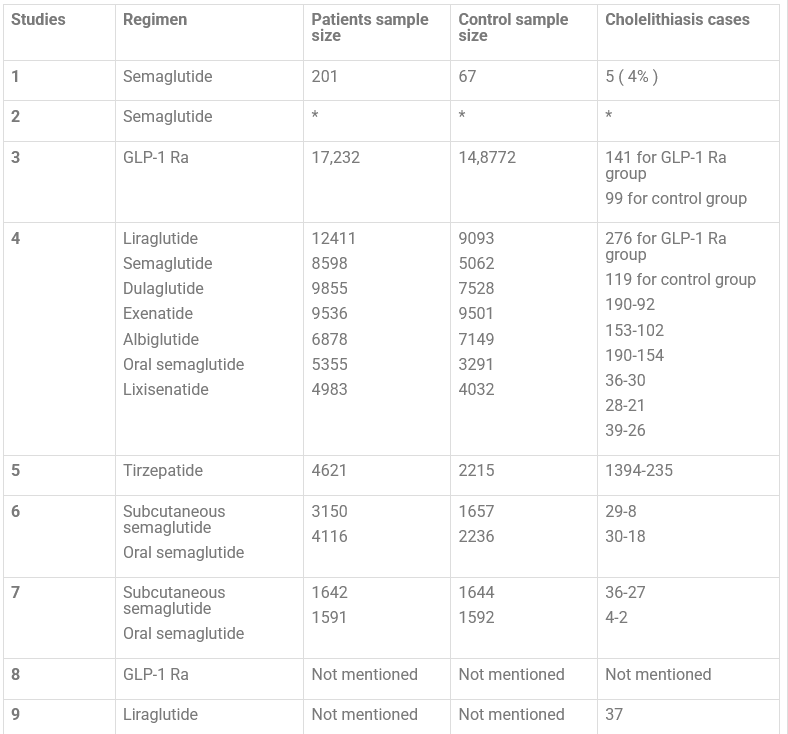 Table: Data derived from the summary of product characteristics, as the manuscripts did not describe these data.
Table: Data derived from the summary of product characteristics, as the manuscripts did not describe these data.