Case Report A rare case of Small Bowel Rupture due to a Richter-like hernia following a pelvic fractureChristos Moutsos1, Christos Farazi-Chongouki 2, Anestis Ninos1, Evangelos Iliopoulos1, Gerasimos Douridas11Surgical Department, Thriasio General Hospital of Elefsina,
2Emergency Department, Thriasio General Hospital of Elefsina
Correspondence Address: Christos Farazi-Chongouki, Dept. of Surgery, Thriasio General Hospital of Elefsina, Athens, Greece, Email: cfarazi@yahoo.grKeywords: traumatic Richter’s hernia, rare pelvic fracture complications, bowel perforation.
Abstract Background. Pelvic fractures are severe injuries often associated with multiple systematic injuries. The most common related complications are: bleeding, retroperitoneal
hematoma, other intra-abdominal and urogenital injuries. There are also rare types of pelvic fracture complications such as ureteral obstruction, bowel entrapment, external iliac
artery injury and open scrotal sac injury. Traumatic hernias on pelvic injuries sites are an extremely rare entity.
Case presentation. A 79-years old woman was admitted to the Accident and Emergency Department suffering from a left pubic rami fracture with active retroperitoneal bleeding
from the left obturator artery following a fall from her own height. Bleeding was managed with intravascular embolization. Her initial uneventful clinical course was discontinued by
relapsing episodes of bowel obstruction and eventually lethal septic syndrome due to bowel perforation due to a Richer-like-hernia as it turned out. Despite rescue laparotomy during
which an enterectomy, lavage and laparostomy were performed the patient passed out in the midst of decaying multiple organ failure syndrome.
Conclusion. Traumatic hernias associated with pelvic fractures complicated with bowel entrapment, is a rarity. Although there are few reports for bowel entrapment into
traumatic cavities of such hernias, the presence of Richter-like traumatic hernia has no record in the literature until today. Every surgeon dealing with trauma should be aware of
the existence of such a rare complication and have a low threshold for early surgical intervention.
Introduction
Pelvic fractures are often caused by high-energy injuries such as those suffered in traffic accidents and falls and account for only 5%-8% of all fractures. Common
complications of pelvic fractures include visceral injury, hemorrhage, genitourinary injury and pulmonary embolism. Traumatic hernia is rare, especially in association with pelvic
fractures. Although the rarity of such cases, it demonstrates a severe course. Therefore, it requires both a proper diagnosis and treatment.1
The first report of a Richter’s hernia was attributed to Fabricius Hildanus in 1606.2 (Figure 1) The description of that case, in his words, translated from the original
Latin origin, goes as follows: “Gangrene resulting from an intestinal hernia with perforation and subsequent cure”.3 A Richter’s hernia is defined as an abdominal hernia, in which
only part of the circumference of the bowel is entrapped and strangulated in the hernia orifice. Although, almost any part of the gastrointestinal tract has been reported in Richter’s
hernias cases, it is the distal ileum that is affected mostly.4-8 August Richter, who first described this condition, states that the precondition for the formation of this particular
hernia is determined by the size and consistency of the hernia orifice. (Figure 3) It must be big enough to ensnare the bowel wall, but small enough to prevent protrusion of an entire
loop of the intestine, and the margin of the hernia’s ring must be firm or, in Richter’s words, “possess strong spring-force”.9Richter’s hernias tend to progress more rapidly to gangrene
than ordinary strangulated ones.10
Besides Richter’s hernia, that is a rare pathology, there are many causes, described in the literature and seen in the everyday clinical practice, for small bowel perforation.
Among others,the most frequent are erosions from duodenal ulcerations, tumors, infection or abscess, Meckel’s diverticulum, hernia with strangulation, inflammatory bowel disease,
mesenteric ischemia, foreign bodies, obstruction, medication or radiation related causes, iatrogenic ruptures and trauma.11
Aim of the present case report description is the presentation of a very rare case of small bowel perforation due to a Richter’s hernia, that has been incarcerated in
a non-anatomical hernia orifice, formed by a pubic bone fracture, following a fall from own height.The review of the literature has shown few similar cases, but there is no
reference in a Richter’s-like traumatic hernia incarceration of small bowel.
Case report
A 79-years old woman presented at the emergency department of our hospital after a fall from her own height. Her medical history included atrial fibrillation and
severe degree mitral valve disease. She was receiving acenocoumarol in a dose of 2 mg/OD. She was unable to stand up and was experiencing severe pain in the pelvis and lower abdomen.
When she arrived in the emergency department, the vital signs were: BP100/70mmHg, HR 110/min, SpO2 98%. The first laboratory examination revealed Hgb 9.3 mg/dl. After resuscitation
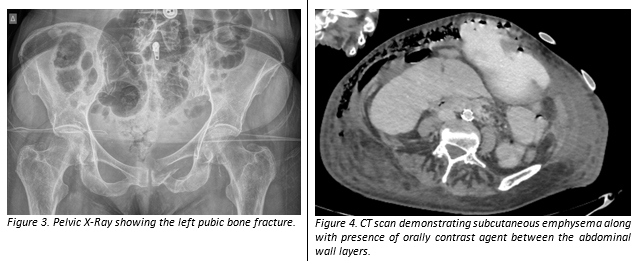
with crystalloids, x-rays showed a pubic bone fracture on the left side. (Figure 3) The second laboratory test reported Hgb 8.1mg/dl. The patient was transfused with RBCs and a
CT-scan was performed, that revealed extensive hematomas in the pelvic floor, the left obturator muscle and in the extraperitoneal place. There was also active bleeding from the
left obturator artery, which was treated with trans-arterial coils embolization. The patient then was hemodynamically and laboratory stabilized. She was admitted to our surgical
department for further observation.
To further assess an easy and clinically useful tool for using PLT2 as a predictor of 30-day survival, we used 225,000/μL, being the mean of the PLT2 covariate, as
derived from the Cox proportional hazards regression univariate analysis. Patients with PLT2 ≥225,000/μL had a hazard ratio (HR) of 0.991 (95% CI: 0.984-0.998) per unit (103/μL)
to succumb within the first 30 days after admission for ICH (HR<1 favors 30-day survival). The result was statistically significant (P=0.048) using the Log-Rank test; the relevant
Kaplan-Meier curve is provided as Figure 2.
At the 7th day of hospitalization, the patient presented symptoms of bowel obstruction (vomiting, abdominal distention) that was conservatively managed with the placement
of nasogastric tube, which decompressed the stomach and the small bowel. The rest of the treatment was entirely supportive with IV fluids, antibiotics, painkillers, metoclopramide and
low-molecular weight heparin. The patient was still passing flatus, so the ileus was rendered to the bed rest due to the pelvic fracture. As she was relieved from her symptoms after
four days and the output of the nasogastric tube was declined (and removed), the patient began on liquid diet per os. At the 17th day of hospitalization, the patient experienced again
symptoms and signs of bowel obstruction. She had a septic profile with fever, elevated white blood cell counts, CRP and atypical abdominal pain without Bloomberg’s sign. There was
a remarkable sign of subcutaneous emphysema, especially in the right side of the abdomen. A CT-scan revealed distended small bowel loops, together with collections in the pelvic
floor and between the layers of the abdominal wall, especially in the left side and presence of free air on both sides of rectus sheath. (Figure 4)
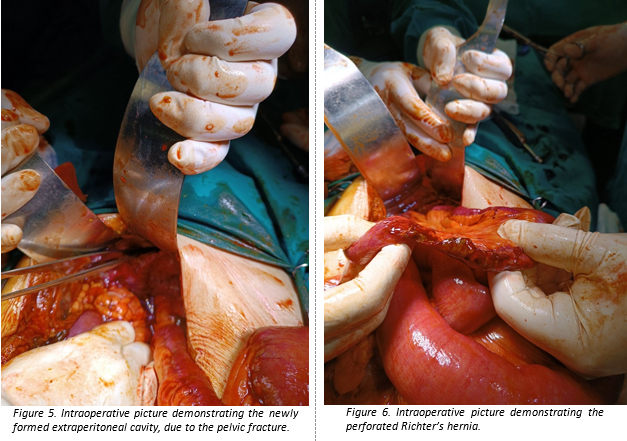
Due to the clinical and radiological findings, an emergency exploratory laparotomy was decided. The midline incision exposed the presence of fecal substance inside
the subcutaneous tissue and the rectus sheath. A Richter-like hernia was discovered inside a cavity created in the abdominal wall by the pelvic fracture, with torsion of the
retroperitoneum and the creation of a non-anatomical orifice, in which there was a circumference small-bowel entrapment and strangulation. (Figure 5)
The bowel was perforated with its substance spilling inside the abdominal wall compartments, especially between the peritoneum and the transversalis fascia. (Figure 6) Surprisingly,
the intraperitoneal cavity was free of any contamination or peritonitis. A segmental enterectomy and side-to-side anastomosis with staplers was performed, as also careful lavage
of the contaminated areas.
A laparotomy with a Bogota-bag technique was performed and vacuum drains were placed in the affected cavity, for daily cleaning care of the abdominal wall and prevention of
abdominal compartment syndrome. The patient was septic and was transferred to the intensive care unit for post-operative monitoring. Unfortunately, she passed away in the 10th
postoperative day, due to multiple-organ failure.
Discussion
The criteria of traumatic hernia proposed by Clain in 1964 are as follows: 1) the hernia must have appeared immediately after trauma and 2) the patient must have consulted a
doctor soon enough for signs of the trauma to be identifiable12. However, many cases that did not fulfill these criteria have subsequently been reported. Therefore, Sahdev proposed
new criteria of traumatic hernia in 1992 as follow: 1) the patient has no history of any hernia, 2) it is obvious that the patient has suffered an injury, 3) the appearance of
herniation can occur at a delayed stage after trauma, and 4) a hernia sac can be present13. Our case apart from the hernia sac includes all of the above criteria.
Sir Frederick Treves, the famous London surgeon, who saved King Edward VII’s life, when he was diagnosed with appendicitis, distinguished Richter’s hernia from herniation of
a Meckel diverticulum, which was classically described be Littre.14 Treves credited Richter with the distinction of having given the first scientific description of this particular
lesion and suggested the term that we all use today.15 For 100 years there was a big confusion among the surgeons about the nomenclature of these hernias. They were described without
a special name or were spoken of it as Littre’s hernia.
Little new information has been added since then and the reports of Treves remain classic and stand still in time.16-17 Approximately, 10% of strangulated hernias are
Richter’s hernias.18-19The diagnosis may be difficult due to lack of specific symptoms and signs and may remain presumptive even after the performance of radiological examinations,
until clearly confirmed in the operational theatre. Vague abdominal pain, slight malaise, nausea and vomiting may be the first symptoms but less common and severe because the
obstruction is rarely complete. Local signs may be absent and if present are easily overlooked. The most constant physical finding remains the tenderness or swelling over a
potential hernia orifice. In late cases, where surgery was performed after days or not at all, with perforation of the strangulated part of the bowel, the results may be devastating
and lethal for the patient, due to gangrene and high toxin load. The good clinical scenario for the patient is the formation of an enterocutaneous fistula, which has been described
first from Hildanus in 16062, as there is no contamination in the intraperitoneal cavity and peritonitis.
However, in the case of our patient, the traumatic hernia led to the development of this fistula between the abdominal wall layers and especially between the peritoneum and
transversalis fascia in a significant quantity of contaminated bowel substance, before its clinical syndrome. A broken pubis led to the formation of a non-anatomical new space or
“orifice”, where the anti-mesenteric border of a loop of the terminal ileum was incarcerated extraperitoneally. Although the time of the incarceration could be combined with the
first symptoms of ileus at the 7th day of hospitalization, it was only when the perforation and the septic profile of the patient ten days after (fever, abdominal pain, metabolic
acidosis, slight tachycardia, slight fall of blood pressure, elevated WBCs and CRP) dictated the need for exploratory laparotomy.
Conclusion
In most cases, pelvic fractures follow a predictable course and the patient heals uneventfully. Traumatic hernia following pelvic fractures is a rare complication, that can
lead to bowel entrapment and perforation extraperitoneally. Since Richter’s hernia is more difficult in diagnosis, a traumatic Richter’s-like hernia will reveal late symptoms of bowel
necrosis and perforation, as described in our case. A high clinical suspicion of this entity may lead to early surgical exploration and prevent severe complications, which may result
in an unfortunate loss of life.
References
1. Ryota Tanaka, Hisashi Nagahara, Kiyoshi Maeda et al. A case of bowel perforation due to traumatic hernia at a pelvic fracture site: a case report and review
of the literature. BMC Surgery (2017) 17:81
2. Fabricius Hildanus. Observationum et Curationum Chirurgicarum Centuriae. Basileae: Sumptibus Ludovici Regis; 1606(1st ed):159.
3. Wolfgang Steinke, Rene Zellweger. (2000). Richter’s Hernia and Sir Frederick Treves: An original clinical experience, review and historical overview.
Annals of Surgery Vol. 232, No. 5, 710-718
4. Tito WA, Allen WC. Richter and Littre Hernia. In: Nyhus JB, Condon RE, eds. Hernia, 3rd edition, Philadelphia: Lippincott; 1989:305–310.
5. Giokas G, Karakousis CP. Richter hernia of the stomach. J Surg Oncol 1998; 69(1):51–53.
6. Duari M. Strangulated femoral hernia: a Richter’s type containing caecum and base of appendix. Postgrad Med J 1966; 42:726–728.
7. Rowe PH, Hunter-Craig C. Richter’s hernia in a direct inguinal sac in a female. J R Coll Surg Edinb 1984; 29:264.
8. Newerla GJ, Connally EF. Gangrenous appendicitis in femoral hernia of Richter’s type. Am J Surg 1943; 61:154–156.
9. Richter AG. Abhandlung von den Bruchen. Gottingen: Johann Christian Dieterich; 1785.
10. Horbach JM. Invagination for Richter-type strangulated hernias. Trop Doct 1986; 16(4):163–168.
11. Brown, C. V. R. (2014). Small Bowel and Colon Perforation. Surgical Clinics of North America, 94(2), 471–475.
12. Clain A. Traumatic hernia. B J Surg. 1964; 51:549–50.
13. Sahdev P, Garramone RR, Desani B. Traumatic abdominal hernia. Report of three cases and review of the literature. Am J Emer Med. 1992;10:237–41.
14. Littre A. Observation sur une nouvelle espece de hernie. Paris: Mem. de l’Acad. Royal des Sciences; 1700:300.
15. Treves F. Richter’s hernia or partial enterocele. Med Chir Tr 1887; 17:149 –167.
16. Kadirov S, Sayfan J, Friedman S, Orda RJ. Richter’s hernia: a surgical pitfall. Am Coll Surg 1996; 182(1):60–62.
17. Fuckiger R, Huber A. Die Richter’sche Hernie. Der Chirurg 1993; 64:822– 826.
18. Frankau C. Strangulated hernias: a review of 1487 cases. Br J Surg 1931; 19:176 –191.
19. Gillespie RW, Glas WN, Mertz GH, Musselman M. Richter’s hernia: its etiology, recognition and management. Arch Surg 1956; 73: 590–594.
Accessibility Bar
visibility_offDisable flashes
titleMark headings
settingsBackground Color
zoom_outZoom out
zoom_inZoom in
remove_circle_outlineDecrease font
add_circle_outlineIncrease font
spellcheckReadable font
brightness_highBright contrast
brightness_lowDark contrast
format_underlinedUnderline links
font_downloadMark links
Reset all optionscached
Χρησιμοποιούμε cookies για να σας προσφέρουμε την καλύτερη δυνατή εμπειρία στη σελίδα μας. Εάν συνεχίσετε να χρησιμοποιείτε τη σελίδα, θα υποθέσουμε πως είστε ικανοποιημένοι με αυτό..
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.
 Besides Richter’s hernia, that is a rare pathology, there are many causes, described in the literature and seen in the everyday clinical practice, for small bowel perforation.
Among others,the most frequent are erosions from duodenal ulcerations, tumors, infection or abscess, Meckel’s diverticulum, hernia with strangulation, inflammatory bowel disease,
mesenteric ischemia, foreign bodies, obstruction, medication or radiation related causes, iatrogenic ruptures and trauma.11
Aim of the present case report description is the presentation of a very rare case of small bowel perforation due to a Richter’s hernia, that has been incarcerated in
a non-anatomical hernia orifice, formed by a pubic bone fracture, following a fall from own height.The review of the literature has shown few similar cases, but there is no
reference in a Richter’s-like traumatic hernia incarceration of small bowel.
Besides Richter’s hernia, that is a rare pathology, there are many causes, described in the literature and seen in the everyday clinical practice, for small bowel perforation.
Among others,the most frequent are erosions from duodenal ulcerations, tumors, infection or abscess, Meckel’s diverticulum, hernia with strangulation, inflammatory bowel disease,
mesenteric ischemia, foreign bodies, obstruction, medication or radiation related causes, iatrogenic ruptures and trauma.11
Aim of the present case report description is the presentation of a very rare case of small bowel perforation due to a Richter’s hernia, that has been incarcerated in
a non-anatomical hernia orifice, formed by a pubic bone fracture, following a fall from own height.The review of the literature has shown few similar cases, but there is no
reference in a Richter’s-like traumatic hernia incarceration of small bowel.
 At the 7th day of hospitalization, the patient presented symptoms of bowel obstruction (vomiting, abdominal distention) that was conservatively managed with the placement
of nasogastric tube, which decompressed the stomach and the small bowel. The rest of the treatment was entirely supportive with IV fluids, antibiotics, painkillers, metoclopramide and
low-molecular weight heparin. The patient was still passing flatus, so the ileus was rendered to the bed rest due to the pelvic fracture. As she was relieved from her symptoms after
four days and the output of the nasogastric tube was declined (and removed), the patient began on liquid diet per os. At the 17th day of hospitalization, the patient experienced again
symptoms and signs of bowel obstruction. She had a septic profile with fever, elevated white blood cell counts, CRP and atypical abdominal pain without Bloomberg’s sign. There was
a remarkable sign of subcutaneous emphysema, especially in the right side of the abdomen. A CT-scan revealed distended small bowel loops, together with collections in the pelvic
floor and between the layers of the abdominal wall, especially in the left side and presence of free air on both sides of rectus sheath. (Figure 4)
At the 7th day of hospitalization, the patient presented symptoms of bowel obstruction (vomiting, abdominal distention) that was conservatively managed with the placement
of nasogastric tube, which decompressed the stomach and the small bowel. The rest of the treatment was entirely supportive with IV fluids, antibiotics, painkillers, metoclopramide and
low-molecular weight heparin. The patient was still passing flatus, so the ileus was rendered to the bed rest due to the pelvic fracture. As she was relieved from her symptoms after
four days and the output of the nasogastric tube was declined (and removed), the patient began on liquid diet per os. At the 17th day of hospitalization, the patient experienced again
symptoms and signs of bowel obstruction. She had a septic profile with fever, elevated white blood cell counts, CRP and atypical abdominal pain without Bloomberg’s sign. There was
a remarkable sign of subcutaneous emphysema, especially in the right side of the abdomen. A CT-scan revealed distended small bowel loops, together with collections in the pelvic
floor and between the layers of the abdominal wall, especially in the left side and presence of free air on both sides of rectus sheath. (Figure 4)
 Due to the clinical and radiological findings, an emergency exploratory laparotomy was decided. The midline incision exposed the presence of fecal substance inside
the subcutaneous tissue and the rectus sheath. A Richter-like hernia was discovered inside a cavity created in the abdominal wall by the pelvic fracture, with torsion of the
retroperitoneum and the creation of a non-anatomical orifice, in which there was a circumference small-bowel entrapment and strangulation. (Figure 5)
The bowel was perforated with its substance spilling inside the abdominal wall compartments, especially between the peritoneum and the transversalis fascia. (Figure 6) Surprisingly,
the intraperitoneal cavity was free of any contamination or peritonitis. A segmental enterectomy and side-to-side anastomosis with staplers was performed, as also careful lavage
of the contaminated areas.
A laparotomy with a Bogota-bag technique was performed and vacuum drains were placed in the affected cavity, for daily cleaning care of the abdominal wall and prevention of
abdominal compartment syndrome. The patient was septic and was transferred to the intensive care unit for post-operative monitoring. Unfortunately, she passed away in the 10th
postoperative day, due to multiple-organ failure.
Due to the clinical and radiological findings, an emergency exploratory laparotomy was decided. The midline incision exposed the presence of fecal substance inside
the subcutaneous tissue and the rectus sheath. A Richter-like hernia was discovered inside a cavity created in the abdominal wall by the pelvic fracture, with torsion of the
retroperitoneum and the creation of a non-anatomical orifice, in which there was a circumference small-bowel entrapment and strangulation. (Figure 5)
The bowel was perforated with its substance spilling inside the abdominal wall compartments, especially between the peritoneum and the transversalis fascia. (Figure 6) Surprisingly,
the intraperitoneal cavity was free of any contamination or peritonitis. A segmental enterectomy and side-to-side anastomosis with staplers was performed, as also careful lavage
of the contaminated areas.
A laparotomy with a Bogota-bag technique was performed and vacuum drains were placed in the affected cavity, for daily cleaning care of the abdominal wall and prevention of
abdominal compartment syndrome. The patient was septic and was transferred to the intensive care unit for post-operative monitoring. Unfortunately, she passed away in the 10th
postoperative day, due to multiple-organ failure.