Case Series Injection of fentanyl patches – a deadly routeMaria Tereza Siavou,1 Aliki Fiska,1 Maria Valeria Karakasi,2 Orthodoxia Mastrogianni,3 Amvrosios Orfanidis,4 Nikolaos Raikos,4 Pavlos Pavlidis2
1 Laboratory of Anatomy, School of Medicine, Democritus University of Thrace,
2 Laboratory of Forensic Sciences, School of Medicine, Democritus University of Thrace
3 Toxicology Laboratory of Forensic Service of Thessaloniki, Ministry of Justice
4 Laboratory of Forensic Medicine and Toxicology, School of Medicine, Aristotle University of Thessaloniki
Abstract
Transdermal fentanyl therapeutic system was developed to provide continuous, controlled, systemic release of fentanyl. Modifying the route of administration of the drug by
violating the appropriate, proposed medical method for the treatment regimen can be fatal. We present four (4) fatal cases of intravenous abuse of fentanyl transdermal patches, which
took place in the wider region of Northern Greece in a short time period. We review the reported cases worldwide and emphasize the importance of public awareness for the
prevention of fatalities.
Key words: fentanyl-related death, intravenous drug abuse, transdermal fentanyl patches
Introduction
Fentanyl is an extremely potent analgesic and anesthetic synthetic opioid, whose chemical properties enable different routes of administration. This novel drug was
synthesized in the 60’s and is widely used since. The development of multiple pharmaceutical dosage forms increased its market dissemination and availability. One of these formulations
was the transdermal therapeutic system (TTS) which provides continuous, controlled, systemic release of fentanyl [1].
Opioids constitute a significant part of the drug abuse problem, including fentanyl abuse, which rapidly increased with the introduction of transdermal patches [2].
The increase in fentanyl-related mortality, both through prescription medication and through illicit use, was attributed to the toxicity of fentanyl, either as a single administration
or in combination with other drugs, to the extent that it was characterized in developed countries, such as the United States of America and Canada, as "fentanyl epidemic" [3], [4].
The drug’s potency and the lack of awareness for the great importance of its proper use intensified the problem in the years following the introduction of fentanyl into the
pharmaceutical market [5].
The high toxicity of fentanyl, combined with its addictiveness, as it produces 50 to 2000 times greater than heroin euphoric symptoms, if IV applicated, has signaled an alert for
the ease with which it can be spread to drug addicts’ circles [6]. To quickly achieve the euphoric level, drug users modify the delivery route of the transdermal patch, in violation
of the drug’s instructions [2]. It should be noted that high toxicity is not the only factor contributing to the increased risk of fentanyl abuse with respect to other opioids;
fentanyl transdermal patch (the 72h regimen) contains a fatal amount of opioid when it is intravenously administrated [7]. The first case of intravenous abuse of a transdermal
fentanyl patch was reported by DeSio and his colleagues [7] in 1993.
We present four (4) fatal cases of intravenous abuse of fentanyl TTS originating from the wider region of Central and Eastern Macedonia and Thrace. Three of these were processed at
the Laboratory of Forensic Medicine and Toxicology of Democritus University of Thrace and the fourth at the corresponding Laboratory of Aristotle University of Thessaloniki.
All cases occurred within three years’ time.
In the light that the reported number of deaths from intravenous fentanyl patches abuse is only 12 worldwide; our report reflects the rare phenomenon of the accumulation of four
fatalities in a short period in a small Greek territory.
Case Presentations
In all cases, the death scene was examined to exclude the possibility of a criminal act, including the position of the deceased. Medical history and clinical records
of the victims and additional information from the deceased's relatives or friendly environment and police investigating authorities was obtained. Later, autopsy was performed to
clarify the cause of death and collect biological samples for toxicological analysis. External examination of the body included recording body weight and height and identifying and
photographing skin features, such as tattoos, venipunctures, recent or old scars, etc. Thorough internal examination of the deceased was performed, during which biological material
(blood, urine, bile) and visceral tissue biopsies were obtained and forwarded, for laboratory documentation of the use of addictive substances. All biological samples were screened
for ethanol and drugs of abuse. For presumptive positive screening tests, confirmatory analysis was performed by Gas Chromatography/Mass Spectrometry (GC-MS).
Case 1
A 46-year-old female of 57 kg weight and 1.66 m height, with a known long history of heroin and ethanol abuse, was found dead at home. Externally, the decedent had a recent venipuncture
on her left arm. An empty Durogesic 12 μg/h package was found in the trash, but no sign of a patch was spotted on her skin and no syringe or other drug IV equipment was discovered.
Presumably, paraphernalia were removed from the scene by co-users, friends, or relatives. During forensic autopsy, the brain was markedly edematous and in the thoracic region there
was pulmonary congestion and edema. From the presumptive screening tests of biological fluids (blood and urine), performed at the Laboratory of Pharmacology of the General University
Hospital of Alexandroupolis, resulted negativity for ethanol, cannabinoids and opiates and positivity for benzodiazepines. After these results, additional confirmatory toxicological
analysis was carried out at the Laboratory of Forensic Medicine and Toxicology of the National and Kapodistrian University of Athens and concluded positivity for fentanyl at a
concentration of 8 ng/mL in blood sample.
Case 2
A 24-year-old man of 81 kg weight and 1.73 m height, with a history of alcoholism and continuous intravenous heroin use over the last four years, was found dead after a day’s search,
at a building under construction. During examination of the scene, we found equipment for intravenous drug use and a used Durogesic 12 μg/h package. An insulin syringe full of
yellowish liquid was observed on his left arm and a tourniquet above it. Additionally, there was evidence of contusions on his left facial, frontal and nasal area, which were not
responsible for his death and attributed to falling on the building materials, where he was found. During autopsy, we observed marked brain edema and severe congestion of the lungs.
Table 1. Review of reported cases of abuse of fentanyl transdermal system with intravenous administration (* 5 out of 23 / 10 out of 112 and 72 out of 242 fatal cases.)
Blood and urine samples were sent for toxicological analysis to the Laboratory of Pharmacology of the General University Hospital of Alexandroupolis, as well as to the Laboratory
of Forensic Medicine and Toxicology of the National and Kapodistrian University of Athens. The presumptive screening tests were positive for benzodiazepines and cannabinoids
and negative for opiates. Biological materials processed by the Laboratory of Forensic Medicine and Toxicology of the National and Kapodistrian University of Athens, were negative
for ethanol and positive for bromazepam, cannabinoids and fentanyl, that was detected and quantified in the blood sample at the concentration of 98 ng/mL. Fentanyl was also
identified in the remnants from the syringe.
Case 3
A 37-year-old man, of 86 kg weight and 1.81 m height, was found dead in his home by his father two days after he had last been known to be alive. The deceased had a history of
hepatic cirrhosis, due to chronic alcoholism and use of addictive substances (opioids, cannabis and benzodiazepines). Tools for intravenous drug use were found at the death scene,
as well as a coffee pot containing a molten plastic residue from a Durogesic transdermal patch. At external examination, we observed a tourniquet in his right upper limb and a
recent venipuncture under it, while old needle marks were seen to both his upper limbs. During forensic autopsy, severe cerebral edema was found, while the lungs were edematous.
The toxicological analysis by the Laboratory of Toxicology of Aristotle University of Thessaloniki was positive for benzodiazepines and positive for fentanyl in blood sample.
Although the fentanyl concentration in the blood was “very high”, quantification was not possible.
Case 4
A 34-year-old man, of 83 kg weight and 1.77 m height, chronic user of addictive substances (heroin, benzodiazepines, cannabis) for at least five years, was found dead in a building
under construction. External examination revealed old needle puncture sites in his upper and lower extremities and a recent venipuncture on his left arm. During forensic autopsy,
acute pulmonary and cerebral edema was found. The results of the toxicological analysis by the Laboratory of Toxicology of Aristotle University of Thessaloniki were positive
for diazepam, nordiazepam, oxazepam, bromazepam, temazepam, 7-amino flunitrazepam and fentanyl in blood sample. In this
case fentanyl was primarily detected, but again quantification was not possible.
Discussion
Fentanyl abuse and related deaths has a young to middle aged male predilection [26]. Accordingly, our cases comprised 3 males and 1 female with ages ranging from 24 to 46 years.
Figure 1. Isolation by heating of the active substance from fentanyl transdermal patch (Case 3).
Figure 2. Intravenous injection of fentanyl (Case 2).
All cases had a known prior history of drug abuse. Information gathered from co-consumers and / or relatives revealed that the supply of fentanyl transdermal patches was
through legal prescription to patients, who were relatives of the deceased. The latter, after illegally obtaining the pharmaceutical preparations, isolated fentanyl by heating
the patch and injected it in their body (Fig. 1, Fig. 2).
In most fentanyl abuse cases reported in the international literature, death comes due to interaction with other toxic substances, mainly ethanol, amphetamine, cocaine, codeine,
benzodiazepines and others [9], [10], [12], [13], [14], [15].
The toxicological analysis of all four cases detected the presence of other addictive substances in addition to fentanyl including cannabinoids and benzodiazepines and so the
intoxication could not be attributed to fentanyl alone. In view of the low concentrations of the accompanying drugs compared to the fentanyl concentration, fentanyl was considered
as the leading substance.
Despite extensive international research efforts, as in Andresen et al. [16] review, it is not possible to determine a marginal level between toxic and non-toxic concentrations
of fentanyl. The determination of the precise antemortem dose of fentanyl with the use of its postmortem concentrations is impossible in cases of abuse [17], and even in cases
of prescriptive therapeutic use [18].
In fact, many factors may play a role in each case: the degree of opioid tolerance is the most important, as it can explain why new users show extremely high concentrations of
the substance and run the risk of a single application of the transdermal patch being fatal [13].
The diversity of postmortem fentanyl concentration levels involves the time elapsed from fentanyl use to the time of death and the possibility of multiple, simultaneous routes of
administration [14] [15] [26]. Postmortem redistribution of fentanyl should also be considered, since completely different pharmacokinetics of the substance is observed in new users [17].
Other idiosyncratic factors may also play a role, such as obesity [16]. As observed from body mass indexes (BMI) none of the decedents in our cases were obese; they were in weight
normal range.
The reported levels of fentanyl (8 and 98 ng/mL for cases 1 and 2 respectively) were consistent with the Anderson and Muto [19] suggestion that “Postmortem blood fentanyl levels
following therapeutic administration can range to 7 µg/L.” Furthermore, the post-mortem fentanyl redistribution phenomenon seems to be enhanced as the drug levels increase [19].
Fentanyl related death occurs from acute respiratory failure, accompanied by severe cerebral and pulmonary edema, as has been observed in all our cases, in accordance with international
literature.
It is also noteworthy that in the death reports associated with fentanyl's abuse, there is a period of accumulation of fatal incidents, ranging from 2 to 55 months [10], [12], [20].
The same plateau was also observed in our cases, considering that three out of four (in the Thrace district) took place in just a three-month period. This observation demonstrates
that probably the information about fentanyl isolation and abuse methods is rapidly spread among drug addicts’ circles.
Another important factor is that transdermal fentanyl patches are relatively easy to obtain. Users can secretly or violently detach them from their chronically ill relatives [13] or
they can obtain them by misleading doctors to multiple prescribing [7], or even remove them from the dead body of cancer patients [21].
In several reported cases of transdermal fentanyl-related deaths, it is not entirely possible to document the precise way of use of the patch. Its intravenous abuse is deduced from
the presence of needle puncture sites on the cadaver, either from testimonies of relatives or friends and "co-users" of the deceased, or when it is the most likely cause of death,
with the method of exclusion [15].
In our literature search, we unearthed 10 reports, with 99 cases of intravenous abuse of fentanyl patches, 94 of which fatal (Table 1). The large study of fentanyl-related deaths in
Germany by Sinicina et al (2017) considerably raises the number of the reported abuse cases, but no further information is available regarding gender and mixed intoxication of the cases.
There is a remarkable proposal, introduced by Reeves & Ginifer [8], highlighting the importance of proper use of transdermal patches after legal prescribing and safe storage, to avoid
the possibility of them being stolen. They also suggested that accounting of the transdermal patches should be legislated, accompanied by the obligation to return the used patches
to make it possible for new ones to be prescribed. The latter method does not find us in agreement, as there is no way to ensure that the transdermal patches have been appropriately used.
Conclusion
Public warning about the danger of fentanyl, targeted on both health care professionals and drug addicts, is crucial to fatalities prevention. In our point of view, more than
monitoring its prescription, bringing the lethal potential of fentanyl abuse to public attention is the most important factor for eliminating its further illegal and uncontrolled use.
References
1. Stanley TH, The fentanyl story, J. Pain. 15 (12) (2014) 1215-1226. Error! Hyperlink reference not valid..
2. Carson HJ, Knight LD, Dudley MH, Garg U, A fatality involving an unusual route of fentanyl delivery: Chewing and aspirating the transdermal patch, Leg. Med. 12 (3)
(2010) 157-159. https://doi.org/10.1016/j.legalmed.2010.03.001.
3. Schumann H, Erickson T, Thompson TM, Zautcke JL, Denton JS, Fentanyl epidemic in Chicago, Illinois and surrounding Cook County, Clin. Toxicol. 46 (6) (2008) 501-506.
https://doi.org/ 10.1080/15563650701877374.
4. Fischer B, Vojtila L, Rehm J, The ‘fentanyl epidemic’ in Canada - Some cautionary observations focusing on opioid-related mortality, Prev. Med. 107 (2018) 109-113.
https://doi.org/10.1016/j.ypmed.2017.11.001.
5. Moon JM, Chun BJ, Fentanyl intoxication caused by abuse of transdermal fentanyl, J. Emerg. Med. 40 (1) (2011) 37-40. https://doi.org/10.1016/j.jemermed.2007.10.075.
6. LaBarbera M, Wolfe T, Characteristics, attitudes and implications of fentanyl use based on reports from self-identified fentanyl users, J. Psychoactive Drugs.
15 (4) (1983) 293-301. https://doi.org/10.1080/02791072.1983.10471966
7. DeSio JM, Bacon DR, Peer G, Lema MG, Intravenous abuse of transdermal fentanyl therapy in a chronic pain patient, Anesthesiology. 79 (5) (1993) 1139-1141.
https://doi.org/10.1097/ 00000542-199311000-00036.
8. Reeves MD, Ginife CLr, Fatal intravenous misuse of transdermal fentanyl, Med. J. Aust. 177 (10) (2002) 552–553.
https://www.mja.com.au/ system/files/issues/177_10_181102/ree10446_fm.pdf.
9. Kuhlman JJ Jr, McCaulley R, Valouch TJ, Behonick GS, Fentanyl use, misuse, and abuse: a summary of 23 postmortem cases, J. Anal. Toxicol. 27 (7) (2003) 499-504.
10. Tharp AM, Winecker RE, Winston DC, Fatal intravenous fentanyl abuse: four cases involving extraction from transdermal patches,
Am. J. Forensic Med. Pathol. 25 (2) (2004) 178–181. https://doi.org/10.1097/01.paf.0000127398.67081.11.
11. Lilleng PK, Mehlum LI, Bachs L, Morild I, Deaths after intravenous misuse of transdermal fentanyl, J. Forensic Sci. 49 (6) (2004) 1364-1366.
https://doi.org/10.1520/jfs04143.
12. Kronstrand R, Druid H, Holmgren P, Rajs J, A cluster of fentanyl-related deaths among drug addicts in Sweden, Forensic Sci. Int. 88 (3) (1997) 185-195.
https://doi.org/10.1016/s0379-0738(97) 00068-6.
13. Jumbelic MI, Deaths with transdermal fentanyl patches, Am. J. Forensic Med. Pathol. 31 (1) (2010) 18-21. https://doi.org/10.1097 /paf.0b013e31818738b8.
14. Woodall KL, Martin TL, McLellan BA, Oral Abuse of Fentanyl Patches (Duragesic): seven case reports, J. Forensic Sci. 53 (1) (2008) 222-225.
https://doi.org/10.1111/j.1556-4029.2007. 00597.x.
15. Sinicina I, Sachs H, Keil W, Post-mortem review of fentanyl-related overdose deaths among identified drug users in Southern Bavaria, Germany, 2005-2014,
Drug Alcohol. Depend. 180 (2017) 286-291. https://doi.org/10.1016 j.drugalcdep.2017.08.021.
16. Andresen H, Gullans A, Veselinovic M, Anders S, Schmoldt A, Iwersen-Bergmann S, Mueller A, Fentanyl: toxic or therapeutic? Postmortem and antemortem blood
concentrations after transdermal fentanyl application, J. Anal. Toxicol. 36 (3) (2012) 182-194. https://doi.org/ 10.1093/jat/bks005.
17. Gill JL, Lin PT, Nelson L, Reliability of postmortem fentanyl concentrations in determining the cause of death, J. Med. Toxicol. 9 (1) (2013) 34-41.
https://doi.org/10.1007/s13181-012-0253-z.
18. McIntyre IM, Gary RD, Estrada J, Nelson JL, Antemortem and postmortem fentanyl concentrations: a case report, Int. J. Legal. Med. 128 (1) (2014) 65-67.
https://doi.org/10.1007/s00414-013-0897-5.
19. Anderson DT, Muto JJ, Duragesic® transdermal patch: postmortem tissue distribution of fentanyl in 25 cases, J. Anal. Toxicol. 24 (7) (2000): 627–634.
https://doi.org/10.1093/jat/ 24.7.627.
20. Daniulaityte R, Juhascik MP, Strayer KE, Sizemore IE, Harshbarger KE, Antonides HM, Carlson RR, Overdose deaths related to fentanyl and its analogs -
Ohio, January-February 2017, MMWR Morb. Mortal. Wkly. Rep. 66 (34) (2017) 904-908. https: // doi.org / 10.15585 / mmwr. mm6634a3.
21. Flannagan LM, Butts JD, Anderson WH, Fentanyl patches left on dead bodies - potential source of drug for abusers, J. Forensic Sci. 41 (2) (1996) 320-321.
https://doi.org/10.1520 /jfs15436j.
22. Jost U, Wolter E, Böhrer H, Mehrfache missbräuchliche intravenöse Injektion von Fentanyl aus einem transdermalen System [Repeated improper intravenous
injection of fentanyl from a transdermal system]. Dtsch Med Wochenschr. 2004 Feb 13;129(7):313-4. German. Error! Hyperlink reference not valid.
23. Martin TL, Woodall KL, McLellan BA, Fentanyl-Related Deaths in Ontario, Canada: Toxicological Findings and Circumstances of Death in 112 Cases (2002–2004),
J. Anal. Toxicol. 30 (8): 603-610 (2006) https://doi.org/10.1093/jat/ 30.8.603
24. Magdalan J, Ciezkie zatrucie na skutek dozylnego wstrzykniecia fentanylu wyekstrahowanego z przezskórnego systemu terapeutycznego--opis przypadku
[Severe nonfatal poisoning after intravenous abuse of transdermal fentanyl--a case report]. Przegl Lek. 2009;66(6):341-2. Polish.
25. Schauer CK, Shand J, and Reynolds TM, The Fentanyl Patch Boil-Up – A Novel Method of Opioid Abuse. Basic Clin Pharmacol Toxicol, 117: 358-359 (2015)
26. Zanon M, Valentinuz E, Montanaro M, Radaelli D, Consoloni L, D’Errico S, Fentanyl transdermal patch: The silent new killer? Forensic Science International:
Reports, 100104. (2020) https://doi:10.1016/j.fsir.2020.100104
Accessibility Bar
visibility_offDisable flashes
titleMark headings
settingsBackground Color
zoom_outZoom out
zoom_inZoom in
remove_circle_outlineDecrease font
add_circle_outlineIncrease font
spellcheckReadable font
brightness_highBright contrast
brightness_lowDark contrast
format_underlinedUnderline links
font_downloadMark links
Reset all optionscached
Χρησιμοποιούμε cookies για να σας προσφέρουμε την καλύτερη δυνατή εμπειρία στη σελίδα μας. Εάν συνεχίσετε να χρησιμοποιείτε τη σελίδα, θα υποθέσουμε πως είστε ικανοποιημένοι με αυτό..
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.
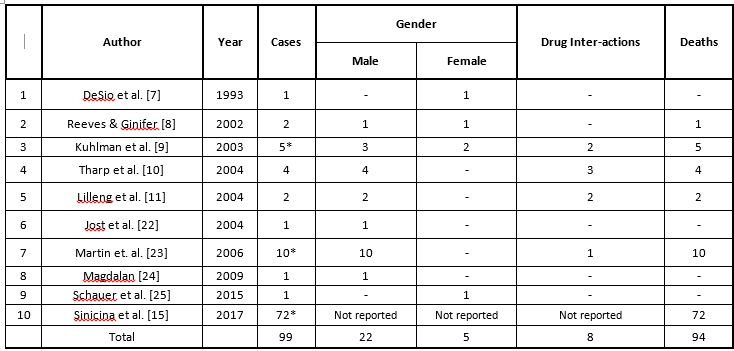 Table 1. Review of reported cases of abuse of fentanyl transdermal system with intravenous administration (* 5 out of 23 / 10 out of 112 and 72 out of 242 fatal cases.)
Blood and urine samples were sent for toxicological analysis to the Laboratory of Pharmacology of the General University Hospital of Alexandroupolis, as well as to the Laboratory
of Forensic Medicine and Toxicology of the National and Kapodistrian University of Athens. The presumptive screening tests were positive for benzodiazepines and cannabinoids
and negative for opiates. Biological materials processed by the Laboratory of Forensic Medicine and Toxicology of the National and Kapodistrian University of Athens, were negative
for ethanol and positive for bromazepam, cannabinoids and fentanyl, that was detected and quantified in the blood sample at the concentration of 98 ng/mL. Fentanyl was also
identified in the remnants from the syringe.
Case 3
A 37-year-old man, of 86 kg weight and 1.81 m height, was found dead in his home by his father two days after he had last been known to be alive. The deceased had a history of
hepatic cirrhosis, due to chronic alcoholism and use of addictive substances (opioids, cannabis and benzodiazepines). Tools for intravenous drug use were found at the death scene,
as well as a coffee pot containing a molten plastic residue from a Durogesic transdermal patch. At external examination, we observed a tourniquet in his right upper limb and a
recent venipuncture under it, while old needle marks were seen to both his upper limbs. During forensic autopsy, severe cerebral edema was found, while the lungs were edematous.
The toxicological analysis by the Laboratory of Toxicology of Aristotle University of Thessaloniki was positive for benzodiazepines and positive for fentanyl in blood sample.
Although the fentanyl concentration in the blood was “very high”, quantification was not possible.
Case 4
A 34-year-old man, of 83 kg weight and 1.77 m height, chronic user of addictive substances (heroin, benzodiazepines, cannabis) for at least five years, was found dead in a building
under construction. External examination revealed old needle puncture sites in his upper and lower extremities and a recent venipuncture on his left arm. During forensic autopsy,
acute pulmonary and cerebral edema was found. The results of the toxicological analysis by the Laboratory of Toxicology of Aristotle University of Thessaloniki were positive
for diazepam, nordiazepam, oxazepam, bromazepam, temazepam, 7-amino flunitrazepam and fentanyl in blood sample. In this
case fentanyl was primarily detected, but again quantification was not possible.
Table 1. Review of reported cases of abuse of fentanyl transdermal system with intravenous administration (* 5 out of 23 / 10 out of 112 and 72 out of 242 fatal cases.)
Blood and urine samples were sent for toxicological analysis to the Laboratory of Pharmacology of the General University Hospital of Alexandroupolis, as well as to the Laboratory
of Forensic Medicine and Toxicology of the National and Kapodistrian University of Athens. The presumptive screening tests were positive for benzodiazepines and cannabinoids
and negative for opiates. Biological materials processed by the Laboratory of Forensic Medicine and Toxicology of the National and Kapodistrian University of Athens, were negative
for ethanol and positive for bromazepam, cannabinoids and fentanyl, that was detected and quantified in the blood sample at the concentration of 98 ng/mL. Fentanyl was also
identified in the remnants from the syringe.
Case 3
A 37-year-old man, of 86 kg weight and 1.81 m height, was found dead in his home by his father two days after he had last been known to be alive. The deceased had a history of
hepatic cirrhosis, due to chronic alcoholism and use of addictive substances (opioids, cannabis and benzodiazepines). Tools for intravenous drug use were found at the death scene,
as well as a coffee pot containing a molten plastic residue from a Durogesic transdermal patch. At external examination, we observed a tourniquet in his right upper limb and a
recent venipuncture under it, while old needle marks were seen to both his upper limbs. During forensic autopsy, severe cerebral edema was found, while the lungs were edematous.
The toxicological analysis by the Laboratory of Toxicology of Aristotle University of Thessaloniki was positive for benzodiazepines and positive for fentanyl in blood sample.
Although the fentanyl concentration in the blood was “very high”, quantification was not possible.
Case 4
A 34-year-old man, of 83 kg weight and 1.77 m height, chronic user of addictive substances (heroin, benzodiazepines, cannabis) for at least five years, was found dead in a building
under construction. External examination revealed old needle puncture sites in his upper and lower extremities and a recent venipuncture on his left arm. During forensic autopsy,
acute pulmonary and cerebral edema was found. The results of the toxicological analysis by the Laboratory of Toxicology of Aristotle University of Thessaloniki were positive
for diazepam, nordiazepam, oxazepam, bromazepam, temazepam, 7-amino flunitrazepam and fentanyl in blood sample. In this
case fentanyl was primarily detected, but again quantification was not possible.
 Figure 1. Isolation by heating of the active substance from fentanyl transdermal patch (Case 3).
Figure 1. Isolation by heating of the active substance from fentanyl transdermal patch (Case 3).
 Figure 2. Intravenous injection of fentanyl (Case 2).
All cases had a known prior history of drug abuse. Information gathered from co-consumers and / or relatives revealed that the supply of fentanyl transdermal patches was
through legal prescription to patients, who were relatives of the deceased. The latter, after illegally obtaining the pharmaceutical preparations, isolated fentanyl by heating
the patch and injected it in their body (Fig. 1, Fig. 2).
In most fentanyl abuse cases reported in the international literature, death comes due to interaction with other toxic substances, mainly ethanol, amphetamine, cocaine, codeine,
benzodiazepines and others [9], [10], [12], [13], [14], [15].
The toxicological analysis of all four cases detected the presence of other addictive substances in addition to fentanyl including cannabinoids and benzodiazepines and so the
intoxication could not be attributed to fentanyl alone. In view of the low concentrations of the accompanying drugs compared to the fentanyl concentration, fentanyl was considered
as the leading substance.
Despite extensive international research efforts, as in Andresen et al. [16] review, it is not possible to determine a marginal level between toxic and non-toxic concentrations
of fentanyl. The determination of the precise antemortem dose of fentanyl with the use of its postmortem concentrations is impossible in cases of abuse [17], and even in cases
of prescriptive therapeutic use [18].
In fact, many factors may play a role in each case: the degree of opioid tolerance is the most important, as it can explain why new users show extremely high concentrations of
the substance and run the risk of a single application of the transdermal patch being fatal [13].
The diversity of postmortem fentanyl concentration levels involves the time elapsed from fentanyl use to the time of death and the possibility of multiple, simultaneous routes of
administration [14] [15] [26]. Postmortem redistribution of fentanyl should also be considered, since completely different pharmacokinetics of the substance is observed in new users [17].
Other idiosyncratic factors may also play a role, such as obesity [16]. As observed from body mass indexes (BMI) none of the decedents in our cases were obese; they were in weight
normal range.
The reported levels of fentanyl (8 and 98 ng/mL for cases 1 and 2 respectively) were consistent with the Anderson and Muto [19] suggestion that “Postmortem blood fentanyl levels
following therapeutic administration can range to 7 µg/L.” Furthermore, the post-mortem fentanyl redistribution phenomenon seems to be enhanced as the drug levels increase [19].
Fentanyl related death occurs from acute respiratory failure, accompanied by severe cerebral and pulmonary edema, as has been observed in all our cases, in accordance with international
literature.
It is also noteworthy that in the death reports associated with fentanyl's abuse, there is a period of accumulation of fatal incidents, ranging from 2 to 55 months [10], [12], [20].
The same plateau was also observed in our cases, considering that three out of four (in the Thrace district) took place in just a three-month period. This observation demonstrates
that probably the information about fentanyl isolation and abuse methods is rapidly spread among drug addicts’ circles.
Another important factor is that transdermal fentanyl patches are relatively easy to obtain. Users can secretly or violently detach them from their chronically ill relatives [13] or
they can obtain them by misleading doctors to multiple prescribing [7], or even remove them from the dead body of cancer patients [21].
In several reported cases of transdermal fentanyl-related deaths, it is not entirely possible to document the precise way of use of the patch. Its intravenous abuse is deduced from
the presence of needle puncture sites on the cadaver, either from testimonies of relatives or friends and "co-users" of the deceased, or when it is the most likely cause of death,
with the method of exclusion [15].
In our literature search, we unearthed 10 reports, with 99 cases of intravenous abuse of fentanyl patches, 94 of which fatal (Table 1). The large study of fentanyl-related deaths in
Germany by Sinicina et al (2017) considerably raises the number of the reported abuse cases, but no further information is available regarding gender and mixed intoxication of the cases.
There is a remarkable proposal, introduced by Reeves & Ginifer [8], highlighting the importance of proper use of transdermal patches after legal prescribing and safe storage, to avoid
the possibility of them being stolen. They also suggested that accounting of the transdermal patches should be legislated, accompanied by the obligation to return the used patches
to make it possible for new ones to be prescribed. The latter method does not find us in agreement, as there is no way to ensure that the transdermal patches have been appropriately used.
Figure 2. Intravenous injection of fentanyl (Case 2).
All cases had a known prior history of drug abuse. Information gathered from co-consumers and / or relatives revealed that the supply of fentanyl transdermal patches was
through legal prescription to patients, who were relatives of the deceased. The latter, after illegally obtaining the pharmaceutical preparations, isolated fentanyl by heating
the patch and injected it in their body (Fig. 1, Fig. 2).
In most fentanyl abuse cases reported in the international literature, death comes due to interaction with other toxic substances, mainly ethanol, amphetamine, cocaine, codeine,
benzodiazepines and others [9], [10], [12], [13], [14], [15].
The toxicological analysis of all four cases detected the presence of other addictive substances in addition to fentanyl including cannabinoids and benzodiazepines and so the
intoxication could not be attributed to fentanyl alone. In view of the low concentrations of the accompanying drugs compared to the fentanyl concentration, fentanyl was considered
as the leading substance.
Despite extensive international research efforts, as in Andresen et al. [16] review, it is not possible to determine a marginal level between toxic and non-toxic concentrations
of fentanyl. The determination of the precise antemortem dose of fentanyl with the use of its postmortem concentrations is impossible in cases of abuse [17], and even in cases
of prescriptive therapeutic use [18].
In fact, many factors may play a role in each case: the degree of opioid tolerance is the most important, as it can explain why new users show extremely high concentrations of
the substance and run the risk of a single application of the transdermal patch being fatal [13].
The diversity of postmortem fentanyl concentration levels involves the time elapsed from fentanyl use to the time of death and the possibility of multiple, simultaneous routes of
administration [14] [15] [26]. Postmortem redistribution of fentanyl should also be considered, since completely different pharmacokinetics of the substance is observed in new users [17].
Other idiosyncratic factors may also play a role, such as obesity [16]. As observed from body mass indexes (BMI) none of the decedents in our cases were obese; they were in weight
normal range.
The reported levels of fentanyl (8 and 98 ng/mL for cases 1 and 2 respectively) were consistent with the Anderson and Muto [19] suggestion that “Postmortem blood fentanyl levels
following therapeutic administration can range to 7 µg/L.” Furthermore, the post-mortem fentanyl redistribution phenomenon seems to be enhanced as the drug levels increase [19].
Fentanyl related death occurs from acute respiratory failure, accompanied by severe cerebral and pulmonary edema, as has been observed in all our cases, in accordance with international
literature.
It is also noteworthy that in the death reports associated with fentanyl's abuse, there is a period of accumulation of fatal incidents, ranging from 2 to 55 months [10], [12], [20].
The same plateau was also observed in our cases, considering that three out of four (in the Thrace district) took place in just a three-month period. This observation demonstrates
that probably the information about fentanyl isolation and abuse methods is rapidly spread among drug addicts’ circles.
Another important factor is that transdermal fentanyl patches are relatively easy to obtain. Users can secretly or violently detach them from their chronically ill relatives [13] or
they can obtain them by misleading doctors to multiple prescribing [7], or even remove them from the dead body of cancer patients [21].
In several reported cases of transdermal fentanyl-related deaths, it is not entirely possible to document the precise way of use of the patch. Its intravenous abuse is deduced from
the presence of needle puncture sites on the cadaver, either from testimonies of relatives or friends and "co-users" of the deceased, or when it is the most likely cause of death,
with the method of exclusion [15].
In our literature search, we unearthed 10 reports, with 99 cases of intravenous abuse of fentanyl patches, 94 of which fatal (Table 1). The large study of fentanyl-related deaths in
Germany by Sinicina et al (2017) considerably raises the number of the reported abuse cases, but no further information is available regarding gender and mixed intoxication of the cases.
There is a remarkable proposal, introduced by Reeves & Ginifer [8], highlighting the importance of proper use of transdermal patches after legal prescribing and safe storage, to avoid
the possibility of them being stolen. They also suggested that accounting of the transdermal patches should be legislated, accompanied by the obligation to return the used patches
to make it possible for new ones to be prescribed. The latter method does not find us in agreement, as there is no way to ensure that the transdermal patches have been appropriately used.