Review Article The Effect of Medical Cannabis on Neurological DisordersSinou Nikoleta1,2, Sinou Natalia 1,2, Koutroulakis Stamatios1, Filippou Dimitrios1,2
1 School of Medicine, National and Kapodistrian University of Athens, Athens, Greece
2 Research and Education Institute in Biomedical Sciences
Corresponding Address: Nikoleta Sinou, 18 Vakhou, Agia Paraskevi, Athens GR-15342, Athens, Greece
email: nikoletta.sinou@gmail.com
Abstract
Introduction: Over the centuries, cannabis has been used for recreational purposes, to produce euphoric effects. However, several studies indicate the
potential of cannabis, used as a therapeutic drug. D9-tetrahydrocannabinol (THC) and cannabidiol (CBD) are the two phytocannabinoids, the basic components of cannabis,
that activate receptors of the endocannabinoid system and can be used as a drug for its activation. Endocannabinoid receptors are mainly expressed on central nerve system (CNS).
Materials and Methods: Detailed research was performed via the PubMed database, using the following keywords: THC, CBD, neurological disorders, psychotropic plant,
medical cannabis.
Results: The aim of this review is to highlight the effect that THC and CBD has on neurodegenerative disorders and in particular, in Parkinson Disease (PD),
Alzheimer Disease (AD) and amyotrophic lateral sclerosis (ALS).
Conclusion: The clinical significance of medical cannabis is great, as it may offer anti-inflammatory, anxiolytic, anti-psychotic effects and act as neuroprotective
for neurodegenerative disorders.
Keywords: THC, CBD, neurological disorders, psychotropic plant, medical cannabis
Introduction
Over the last few decades, cannabis products have become popular among young adults for recreational purposes, to produce euphoric effects. However, over the
decades, several studies have investigated the wide use of cannabis in medicine [1]. Cannabis Sativa, commonly known as cannabis, has been used for thousands of years
as medical plant for recreational and therapeutic or medicinal purposes.
According to various targeted commercial purposes, cannabis plants have been under hybridization into hundreds of strains. They are classified under various classification
methods depending on their botanical morphology, subjective effects, chemotoxins and other factors. Cannabis plant contains more than 550 phytochemicals, including
120 identified phytocannabinoids [2]. The primary psychoactive cannabinoid in the cannabis plant is D9-tetrahydrocannabinol (THC), which is mainly
produced in the leaves and flower buds of cannabis plant [3]. Additional cannabinoids, such as cannabinol and Δ8-tetrahydrocannabinol, are also present in Cannabis Sativa,
but in a smaller amount than THC. Moreover, some other basic, but non-psychoactive phytocannabinoids are cannabidiol (CBD), cannabichromene (CBC) and cannabigerol (CBG).
Cannabis plants have different concentration of each of these phytochemicals in each of their part. CBD is about 10% active ingredient, whereas THC about 90% and thus
CBD is considered to be non-psychoactive. However, it’s non-psychotropic effect can alter when the ratio of THC and CBD is above 1:1. Recent studies have shown that
CBD has anxiolytic, anti-inflammatory and antipsychotic action [1,4].
The role of these phytocannabinoids is to bind to the cannabinoid receptors (CB1 and CB2), as well as to other receptor systems, via a mechanism that will be discussed
below. The CB1 receptor is the most common receptor of the central nervous system and is highly expressed in hippocampus, ganglia and cerebellum. Also, CB2 receptor
is expressed in high levels in the periphery, spleen and thymus. Therefore, phytocannabinoids regulate many procedures in neurogenesis and central and peripheric nervous system [3,5].
This review aims to examine the use of the medical cannabis in the neurodegenerative disorders.
Materials and Methods
Detailed research was conducted through the published bibliography via PubMed database. The keywords used for the search were THC, CBD, neurological disorders,
psychotropic plant, medical cannabis. To ensure accuracy and adequacy, information was gathered through a common data extraction form designed for the aforementioned
keywords. The research study adhered to the guidelines of PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews),
a comprehensive approach for conducting scoping reviews. Specifically, as regards the PRISMA, the records that were initially identified through PubMed search were 35.
Additionally, 6 relevant records were obtained through a thorough review of similar articles that accompanied each of the initials records. The final number of
screened records was 41. A total of 16 full-text articles were assessed for eligibility, resulting in the exclusion of 25 articles, titles, and abstracts that
were not relevant with the conducted research. Hence, the specific article is based on the information retrieved from 16 reliable references (Figure 1).
Figure 1: The Effect of Medical Cannabis on Neurodegenerative Disorders, Prisma
Results
Cannabinoids and the endocannabinoid system: Cannabinoids, that are produced endogenously,endocannabinoid receptors and their metabolite enzymes
consist the endocannabinoid system (ECS) which regulates many procedures such as hunger, memory, pain, neurogenesis
and the central nervous system (CNS). CB1 receptor is a G-protein coupled receptor (GPCR), mostly expressed in the brain, as we mentioned above. CB2 receptor is also
a GPCR that is highly expressed in periphery and in spleen and thymus and therefore, has a significant role in the immune system. The lipids anandamide (the ethanolamide
of arachidonic acid) and 2-arachidonoylglycerol (2-AG), are the two known endocannabinoids that activate GPCRs, several ion channels and nuclear receptors. Hydrolases
and lipases are the metabolite enzymes that are involved in biosynthesis and inactivation of endocannabinoids [6-8].
As we mentioned above, CB1 receptor have been detected in high levels in hippocampus, basal ganglia, prefrontal cortex and cerebellum. The location of CB1 receptor in
these tissues proves the significant role of cannabinoid system in the motor and cognitional function. On the contrary, CB2 receptors have a more restricted distribution
and have been found in the periphery, thymus and spleen, in cerebellum and in few brain neurons, as well. However, CB2 receptors are found in low levels in healthy brain,
as they are increased in inflammation [1,9].
The expression and localization of these two receptors in CNS identify the implication of cannabinoid system in many pathophysiological procedures of the neurons and in
neurodegenerative disorders. Phytocannabinoids in C. Sativa, including THC and CBD, are used for many therapeutic effects. Recent studies have proven that although,
THC activates CB1 and CB2 receptors, CBD modulates the activity of both these receptors and metabolite enzymes of endocannabinoids. Also, it can modulate THC’s effects
on CB1 receptor. Therefore, CBD can have either a negative allosteric modulation or an adaptogen, depending on the location that it acts [6,9,10].
CBD has shown great efficacy as an antipsychotic, anti-seizure, anti-inflammatory and anxiolytic, as it activates endocannabinoid receptors and reduces OS and inflammation.
CBD is significantly used as neuroprotective of neurodegenerative diseases and in particular, Parkinson disease (PD) and Alzheimer disease (AD) [11].
Neurodegenerative diseases: Neurodegenerative disorders consist one of the most recent causes of death worldwide. The pathophysiology of neurodegenerative diseases
is the oxidative stress (OS) and the inflammation that cells undergo [12]. In these diseases and in particular in PD and AD, pathological genes express altered proteins
which undergo a procedure of unfolding and form β-structures. Amyotrophic lateral sclerosis (ALS) is also one of the common neurodegenerative disorders. These structures
self-aggregate and represent a-synuclein in PD and tau proteins (TAU) in AD. Thus, neuroinflammation and nerve cell loss are the following procedures that effect
negatively motor function and cognition. Cells are protected from OS by producing cytoprotective enzymes, regulated by Nrf2 (nuclear factor erythroid 2-related factor 2).
Nrf2 has an anti-inflammatory action and regulates hemostasis, in several pathological mechanisms of neurological diseases and thus, it consists a novel therapeutic product [5].
Recent studies have shown that CBD increases the expression of Nrf2 activators and thus, Nrf2 activity. Therefore, CBD’s anti-inflammatory, antioxidant and anxiolytic
actions are manifested through Nrf2 activation [3,13].
Medical cannabis and Parkinson Disease: PD is a major neurodegenerative disorder that affects mostly the elderly and is characterized by the dysfunction and
degeneration of the extrapyramidal system. In specific, the primary locus of the disease is the loss of dopaminergic neurons in the substantia nigra. The loss of
dopamine levels has as a result the initiation of motor symptoms. Moreover, patients with PD present bradykinesia, stiffness and slow rhythmic tremors. As regards
the nonmotor symptoms, patients exhibit depression, psychosis and difficulties in cognition. As we mentioned above, nerve cells undergo inflammation and OS [14].
In addition, recent studies have proven the dysfunction of endocannabinoid system in PD. Therefore, drugs that target endocannabinoid system have been shown to reduce
PD’s symptoms. According to studies, THC relieves partially, patients from motor difficulties, as it enhances physical activity and hand-eye coordination and also,
reduces motor symptoms such as tremors, rigidity and bradykinesia [15,16].
In clinical studies, CBD treatment diminished rapid eye-movement and improved patients’ sleep behavior. In particular, optic nerve and impulse are synchronized with
the optic stimulus and the eyes’ tremor is reduced. CBD reduces the fourth stage of sleep and the brain activity and patients present diminished dream occurrences [9,14].
Medical Cannabis and Alzheimer Disease: Alzheimer disease is a chronic neurodegenerative disorder that affects central nerve system and is characterized by memory
weakening, declining subsequently cognitive functions of the patient. In particular, the cause of AD is a combination of many pathological procedures, depending on
both genetic and environmental factors. The main causes of AD are the aggregation of β-amyloid plaques (Aβ), leading to loss of synapses and lesions. These lesions
are characterized by many inflammatory mediators, produced by brain cells and neurons, which undergo neuroinflammation and OS. Recent studies have proven that CB1 and
CB2 cannabinoid receptors are expressed in senile plaques of AD patients. However, in brain areas of microglia activation CB1 and CB2 receptors are significantly reduced,
with the CB2 to become highly dysregulated. Therefore, cannabinoids, THC and CBD, act positively on AD brain, preventing brain’s neurodegeneration [1,3,16].
In particular, a mix of THC-CBD drugs has been indicated to decrease the accumulation of amyloid-beta plaques and thus, to impair AD symptoms. However, this has primarily
been observed in animal models. CBD acts as neuroprotective, anti-oxidative and anti-apoptotic suppressing Aβ peptide toxicity. However, THC can cause confusion,
dizziness, and worsening cognitive impairment in elderly patients, which may limit its use in AD [2,9].
Medical Cannabis and Amyotrophic Lateral Sclerosis: Amyotrophic lateral sclerosis (ALS), also known as Lou Gehrig’s disease, is a progressive neurodegenerative disorder
that affects nerve cells in the brain and spinal cord, leading to loss of muscle control. The exact causes of ALS have not yet been cleared. Recent studies have proven
that neuroinflammation, OS, glutamate-induced excitotoxicity and cytotoxicity are responsible for the disease. Medical cannabis can pharmacological potentials for
symptom relief in ALS patients. Some research suggests that cannabinoids might reduce glutamate toxicity, potentially offering neuroprotective benefits [2,16].
ALS patients often experience significant pain due to muscle spasticity, cramps, and joint discomfort. Cannabis, particularly THC, is known for its analgesic
properties and can help alleviate chronic pain. Moreover, cannabinoids may reduce muscle stiffness and spasms, Sleep disturbances and anorexia [3,9].
Conclusion
Cannabis has been used for decades for recreational purposes, to produce euphoric effects. However, hundreds of studies and experiments through the years, have
indicated the medical aspect of cannabis and it’s use for therapeutic option in neurodegenerative disorders, such as ALS, PD and AD. In particular, these diseases are
characterized by the abnormal accumulation of mutant or damaged proteins, forming plaques that lead to brain dysfunction.
Endocannabinoid system has a significant role in many procedures and regulates many pathways such as neurogenesis, CNS, hunger, pain, sleep and memory, through CB1 and
CB2 receptors that are mainly expressed in nerve cells. Medical cannabis, THC and CBD, can imitate endocannabinoids and act as neuroprotective, antipsychotic, anxiolytic
and anti- inflammatory, consisting therefore, a powerful therapeutic drug slowing the progression of these neurodegenerative diseases. In particular, THC has shown
potentials for cognitive improvement, while CBD for diminishing spasticity, rigidity and sleep disturbances.
However, clinical and animal studies over the years, indicate have brought to light some concerns and adverse effects of cannabis use, such as addiction, legacy issues,
drug interaction or impairment of the disease. To conclude, data insufficiency, access issues and small-scale clinical trials should make cannabis be used cautiously
until more evidence and clinical studies be confirmed.
References
1. Cohen, K., Weizman, A., & Weinstein, A. (2019). Positive and Negative Effects of Cannabis and Cannabinoids on Health. Clinical pharmacology and therapeutics,
105(5), 1139–1147. https://doi.org/10.1002/cpt.1381
2. Viana, M. B., de Aquino, P. E. A., Estadella, D., Ribeiro, D. A., & Viana, G. S. B. (2022). Cannabis sativa and Cannabidiol: A Therapeutic Strategy for
the Treatment of Neurodegenerative Diseases?. Medical cannabis and cannabinoids, 5(1), 207–219. https://doi.org/10.1159/000527335
3. Leinen, Z. J., Mohan, R., Premadasa, L. S., Acharya, A., Mohan, M., & Byrareddy, S. N. (2023). Therapeutic Potential of Cannabis: A Comprehensive Review of
Current and Future Applications. Biomedicines, 11(10), 2630. https://doi.org/10.3390/biomedicines11102630
4. Mirlohi, S., Bladen, C., Santiago, M., & Connor, M. (2022). Modulation of Recombinant Human T-Type Calcium Channels by Δ9-Tetrahydrocannabinolic Acid In Vitro.
Cannabis and cannabinoid research, 7(1), 34–45. https://doi.org/10.1089/can.2020.0134
5. Mücke, M., Phillips, T., Radbruch, L., Petzke, F., & Häuser, W. (2018). Cannabis-based medicines for chronic neuropathic pain in adults. The Cochrane
database of systematic reviews, 3(3), CD012182. https://doi.org/10.1002/14651858.CD012182.pub2
6. Cristino, L., Bisogno, T., & Di Marzo, V. (2020). Cannabinoids and the expanded endocannabinoid system in neurological disorders. Nature reviews. Neurology,
16(1), 9–29. https://doi.org/10.1038/s41582-019-0284-z
7. Elmes, M. W., Kaczocha, M., Berger, W. T., Leung, K., Ralph, B. P., Wang, L., Sweeney, J. M., Miyauchi, J. T., Tsirka, S. E., Ojima, I., & Deutsch, D. G. (2015).
Fatty acid-binding proteins (FABPs) are intracellular carriers for Δ9-tetrahydrocannabinol (THC) and cannabidiol (CBD). The Journal of biological chemistry, 290(14),
8711–8721. https://doi.org/10.1074/jbc.M114.618447
8. Cherry, A. L., Wheeler, M. J., Mathisova, K., & Di Miceli, M. (2024). In silico analyses of the involvement of GPR55, CB1R and TRPV1: response to THC,
contribution to temporal lobe epilepsy, structural modeling and updated evolution. Frontiers in neuroinformatics, 18, 1294939. https://doi.org/10.3389/fninf.2024.1294939
9. Suryadevara, U., Bruijnzeel, D. M., Nuthi, M., Jagnarine, D. A., Tandon, R., & Bruijnzeel, A. W. (2017). Pros and Cons of Medical Cannabis use by People with
Chronic Brain Disorders. Current neuropharmacology, 15(6), 800–814. https://doi.org/10.2174/1570159X14666161101095325
10. Landucci, E., Mazzantini, C., Lana, D., Davolio, P. L., Giovannini, M. G., & Pellegrini-Giampietro, D. E. (2021). Neuroprotective Effects of
Cannabidiol but Not Δ9-Tetrahydrocannabinol in Rat Hippocampal Slices Exposed to Oxygen-Glucose Deprivation: Studies with Cannabis Extracts and Selected Cannabinoids.
International journal of molecular sciences, 22(18), 9773. https://doi.org/10.3390/ijms22189773
11. Bernal-Chico, A., Tepavcevic, V., Manterola, A., Utrilla, C., Matute, C., & Mato, S. (2023). Endocannabinoid signaling in brain diseases: Emerging relevance of
glial cells. Glia, 71(1), 103–126. https://doi.org/10.1002/glia.24172
12. Gao, Y., Zhuang, Z., Gao, S., Li, X., Zhang, Z., Ye, Z., Li, L., Tang, C., Zhou, M., Han, X., & Li, J. (2017). Tetrahydrocurcumin reduces oxidative stress-induced
apoptosis via the mitochondrial apoptotic pathway by modulating autophagy in rats after traumatic brain injury. American journal of translational research, 9(3), 887–899.
13. Filippini, G., Minozzi, S., Borrelli, F., Cinquini, M., & Dwan, K. (2022). Cannabis and cannabinoids for symptomatic treatment for people with multiple
sclerosis. The Cochrane database of systematic reviews, 5(5), CD013444. https://doi.org/10.1002/14651858.CD013444.pub2
14. Crippa, J. A. S., Hallak, J. E. C., Zuardi, A. W., Guimarães, F. S., Tumas, V., & Dos Santos, R. G. (2019). Is cannabidiol the ideal drug to treat non-motor
Parkinson’s disease symptoms?. European archives of psychiatry and clinical neuroscience, 269(1), 121–133. https://doi.org/10.1007/s00406-019-00982-6
15. Costa, A. C., Joaquim, H. P. G., Pedrazzi, J. F. C., Pain, A. O., Duque, G., & Aprahamian, I. (2022). Cannabinoids in Late Life Parkinson’s Disease and Dementia:
Biological Pathways and Clinical Challenges. Brain sciences, 12(12), 1596. https://doi.org/10.3390/brainsci12121596
16. Pathak, S., Jeyabalan, J. B., Liu, K., Cook, P., Lange, B., Kim, S., Nadar, R., Ward, K., Watts Alexander, C. S., Kumar, A., Dua, K., Moore, T., Govindasamy,
J., & Dhanasekaran, M. (2024). Assessing effects of Cannabis on various neuropathologies: A systematic review. Journal of Ayurveda and integrative medicine, 15(3),
100911. https://doi.org/10.1016/j.jaim.2024.100911
Accessibility Bar
visibility_offDisable flashes
titleMark headings
settingsBackground Color
zoom_outZoom out
zoom_inZoom in
remove_circle_outlineDecrease font
add_circle_outlineIncrease font
spellcheckReadable font
brightness_highBright contrast
brightness_lowDark contrast
format_underlinedUnderline links
font_downloadMark links
Reset all optionscached
Χρησιμοποιούμε cookies για να σας προσφέρουμε την καλύτερη δυνατή εμπειρία στη σελίδα μας. Εάν συνεχίσετε να χρησιμοποιείτε τη σελίδα, θα υποθέσουμε πως είστε ικανοποιημένοι με αυτό..
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.
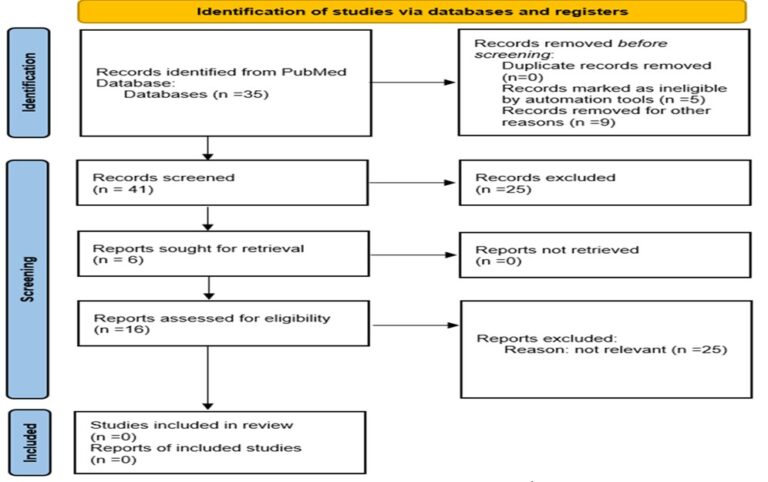 Figure 1: The Effect of Medical Cannabis on Neurodegenerative Disorders, Prisma
Figure 1: The Effect of Medical Cannabis on Neurodegenerative Disorders, Prisma