REVIEWThe role of medical cannabis in the cancer-related pain treatmentSinou Natalia 1,3, Sinou Nikoleta 2,3, Filippou Dimitris 3,4
1 Medical Graduate, National and Kapodistrian University of Athens, Medical School
2 Medical student, National and Kapodistrian University of Athens, Medical School
3 Research and Education Institute of Biomedical Science
4 Surgery, National and Kapodistrian University of Athens, Medical School
Correspondece Address: Natalia Sinou, National and Kapodistrian University of Athens, Medical School, sinou.natalia@gmail.com
Abstract
Introduction: Pain is among others, one of the most common symptoms in patients facing malignancies. The pain may have a major negative impact on their quality of
everyday life. Currently, the gold standard in the treatment of cancer-related pain suggested by WHO are the opioids. However, besides their multiple side effects, there is
a small but significant number of patients that are not relief from pain using these drugs. Thus, there is a need of incorporating different drugs in the treatment of the
cancer-related pain.
Materials and Methods: The aim of this review is to examine the potential of using medical cannabis in the treatment of pain caused by cancer, as long as it’s side and adverse
effects.
Results: Detailed research was conducted via the PubMed database using the keywords: “medical”, “cannabis”, “cancer” and “pain”
Conclusion: Current evidence for the use of cannabis and cannabinoids to relief cancer pain is weak, because of the existence of multiple adverse effects that cannot be
overviewed. However, there is some evidence that indicate that medical cannabis could potentially be beneficially used as an adjunct to the already applying therapy. Further
research needs to be done in this field of medicine in order to incorporate medical cannabis in guidelines for cancer pain management.
Keywords: Medical, Cannabis, Cancer, Pain
Introduction
It is common for patients who face cancer to experience multiple debilitating symptoms including nausea, anxiety, stress and mainly pain. In fact, pain in cancer
patients is extremely common, particularly in advanced stages of the disease, with a prevalence exceeding 70%. There are multiple reasons for which patients who encounter
cancer may experience pain. Pain may arise from the malignancy itself or it may be e result from the therapy against the disease. It can also be related to other comorbid
illness or situation (1), (2). From now on, in this review the pain is defined as the pain related to the malignancy itself and does not correlate with the therapy or any
other coexisting disease.
Although there is a lack of robust clinical data, the usage of cannabis products has been approved in multiple countries for certain medical indications resistant to standard
therapy, including nabilone for chemotherapy-induced vomiting and nausea. Therefore, an extend new field of exploration was the use of the medical cannabis in the treatment
of cancer induced symptoms, such as chemotherapy related nausea, anxiety, depression, insomnia anorexia and most of all cancer related pain.
Cannabis is a plant-based substance made from multiple species within genus Cannabis. Cannabidiol (CBD) is a phyto-alkaloid derived from plants in the Cannabaceae family
and genus Cannabis. According to the various targeted commercial purposes, cannabis plants have been under hybridization into hundreds of strains. There are various
classification methods depending on their botanical morphology, subjective effects, chemotaxines and many other factors. Among all the cannabis components 9-delta-tetrahydrocannabinol
(THC) and cannabidiol (CBD) are the most abundant and as a result the most well studied cannabionoids. Apart from CBD and THC, cannabis constitutes of more than 500 organic
compounds of which more than 100 belong to cannabinoid family. In addition to terpenes and flavonoids the interaction and the effect of the cannabionoids exert their
affection on the endocannabinoid system (3). CBD may comprise even 90% of the plant extract, depending on the species and the extract procedure, along with many addable
terpines and cannabinoids, including tetrahydrocannabinol (THC) (4). Currently cannabinoids drugs exist in synthetic THC form as nabilone and in an approximate 1:1 ratio
THC:CBD plant extract as nabixomols (3). However, THC has psychoactive properties that provoke intoxication and impairment, limiting the use of this drug. On the contrary,
CBD is no psychoactive and thus it does not lie under this restriction (4).
The aim of this review is to examine the use of the medical cannabis in the confrontation of the pain related to malignancy.
Materials and Methods
Detailed research was conducted through the published bibliography via PubMed database. The keywords used for the search were “medical”, “cannabis”, “in”, “cancer”
and “pain”. Data were extracted utilizing a common data elicitation form, using the aforementioned keywords. The study was made with respect to the PRISMA 2020 flow diagram for
new systematic reviews which included searches of databases, registers and other sources guidelines. Specifically, as regards the PRISMA, the records that were initially identified
through PubMed search were 124. These results derived after applying a filter of the last 5 years. There were 3 additional ones through review of references. Also, the full text
articles assessed for eligibility were 14, and the records excluded articles, title and abstract non relevant were 110. There was 1 extra suitable article derived from the similar
articles. All the reports assessed for eligibility were relevant, but 1 of them was written in german, so it was excluded. No duplicates were found. Finally, 17 references
fulfilled the above-mentioned criteria and used in the present work.
Figure 1: PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources **: title and abstract non relevant
Results
There have been conducted several studies examining the use of medical cannabis in the treatment of cancer-related pain.
According to a systematic review and meta-analysis by Boland et al (5) (Boland EG, Bennett MI, Allgar V, Boland JW. Cannabinoids for adult cancer-related pain: systematic
review and meta-analysis), there was not a positive effect by using neither nabiximols nor oromucoal spray (with 1:1 CBD:THC) on the NRS (Numeric Rating Scale) for pain intense
score comparing to the placebo. However, as far as it concerns the adverse effects, the meta-analysis suggests significantly higher odds of somnolence and dizziness in cannabinoid
group. A higher but not statistically significant odds of nausea and vomiting in the cannabinoid group is also reported. None of the studies included in the aforementioned
metanalysis indicated beneficial use of cannabinoids, thus cannabinoids are not recommended for the cancer-related pain management. Similar are the results arising from another
study (Safi K, Sobieraj J, Błaszkiewicz M, Żyła J, Salata B, Dzierżanowski T. Tetrahydrocannabinol and Cannabidiol for Pain Treatment-An Update on the Evidence.) (6)
However, there is a systematic review and meta-analysis by Wang L. (7) (Wang L, Hong PJ, May C, Rehman Y, Oparin Y, Hong CJ, Hong BY, AminiLari M, Gallo L, Kaushal A, Craigie S,
Couban RJ, Kum E, Shanthanna H, Price I, Upadhye S, Ware MA, Campbell F, Buchbinder R, Agoritsas T, Busse JW. Medical cannabis or cannabinoids for chronic non-cancer and cancer
related pain: a systematic review and meta-analysis of randomised clinical trials.) which indicates that not-inhaled medical cannabis and cannabinoids result in a tiny benefit in
pain alleviation, physical function and sleep quality, along with various temporary side effects, compared to a placebo.
Discussion
Opioids in reducing cancer pain: According to the World Health Organisation (WHO) the first step of the analgetic ladder for moderate to severe cancer pain management is the use
of opioids. In clinical practice, the majority of cancer patients is going to deal with the cancer pain by using the opioids. However, there is a small but significant number of
patients that will not have adequate pain relief. Therefore, there is a crucial need for new pain-relieving methods and analgesics, supplementary to opioids to alleviate the pain
of the patients with insufficient pain relief of cancer pain. However, opioids are associated with multiple unwanted side effect including tolerance and dependance, chronic constipation,
loss of appetite, nausea, respiratory depression, sedation and drug induced hyperalgesia. As a result, their clinical use is limited (8).
Pharmacokinetics: The pharmacokinetics of cannabis and cannabinoids are different and depend on the dosage form. Cannabinoids are lipophilic and have a great width of distribution.
THC is known to cross into placenta and breast milk. There are no data to indicate the presence of CBD or metabolites in human milk, although, animal studies highlight embryofetal
developmental toxicity.
Cannabinoids are metabolized in the liver by the cytochrome P450 (CYP) isoenzymes using either hydroxylation or oxidation. After that, they are further metabolized by glucuronidation.
The drug is finally excreted by both urine and feces, after the augment in solubility postmetabolism. THC is largely metabolized by isoenzymes CYP2C19, CYP2C9, and CYP3A4
and the CBD is predominantly metabolized by CYP2C19 and CPY3A4, but also CYP1A1, CYP1A2, CYP2C9, and CYP2D6. It is also suggested by in vitro data that CBD acts like an inhibitor to
p-glycoprotein-mediated drug transport and substrates of uridine 5’-diphospho-glucuronosyltransferase 1A9 and T2B7 (9).
Dosage: The ideal dosage would be the one that would manage effective pain relief without any or at least any intolerable side effect (10). The complicity of the pharmacology,
the variety of the capacities and the amounts of cannabinoids in the products, lead to the inability of the traditional pattern of dose guidance to be used in cannabis. The aforementioned
factors in addition to the existence of other active compounds (flavonoids, terpenoids) and the lack of evidence based clinical trials and studies evaluating dosage forms, doses
and finally the interval between dosages depending on each indication, make it incapable for a safe and efficient dose to be recommended (9).
Furthermore, every patient does not response to therapy same with other patients with the same disease. The response to the treatment depends on other medications, prior exposure
and tolerance to the drug, coexisting diseases, food and the metabolism of the patient itself. Therefore, there is only a rough dosage guideline available and dose should be
personalized for every patient. The gold standard is the titration, same as in every drug, beginning in a low dosage and titrating to the beloved response. This should also be
applied because many of the undesired effects, such as fatigue, dizziness and psychotropic effects, start at an early low dose and tolerance develops overtime.
Cannabis and cannabinoids in patients with cancer: It is common for cannabis products to be used in the treatment of cancer patients. The symptoms that may be treated with the usage
of cannabis and cannabinoids products are multiple such as chemotherapy related nausea and vomiting (21%) stress-anxiety (20%), depression-insomnia (9%), loss of appetite-weight gain
(12%), well-being (17%), treatment of malignancy (4%) and pain (15%) (9).
Adverse effects and side effects: The two main cannabinoids of cannabis are ∆9-tetrahydrocannabinol (∆9-THC) and cannabidiol (CBD). There is a hesitancy in prescribing cannabis for
medicinal use. This is due to the undesirable psychotropic effects of the constituent (∆9-THC) as well as due to other side effects of this substance such as tachycardia, altered
cognitive perception, anxiety and other behavioral issues. Moreover, ∆9-THC may provoke an alteration in the immune system function, augmenting the susceptibility of a patient to
microbial infections. Further, despite the established anti-cancer capacities of ∆9-THC, this cannabinoid has been accused to provoke tumor growth, metastasis and invasion in
some cancer cell types. In breast tumor for instance, ∆9-THC mediated tumor increase and metastasis was related to the inhibition of the anti-tumor specific immune responses in
vivo. Finally, studies demonstrate that cannabis is linked with the evident reduced efficiency of immune checkpoint inhibitors. ∆9-THC has a maximum tolerated daily dose of 15-90 mg
in adult patients approximately, and this small dose requires an ongoing individualized adjustment to make sure that the adverse effects are tolerated to each patient.
Concerning CBD in some cases it is believed that it may cause somnolence and fatigue. However, not permanent or serious adverse effects (such as life-threatening, hospitalization
or surgery requiring interventions, temporary or permanent disability and death) were mentioned (11). Moreover, CBD crosses the placenta and reaches the breast milk, so it is of
grave significance to abstain while pregnant or postpartum/ breast-feeding. Further, due to accumulation, it is highly possible for CBD to cause hepatotoxicity (12). Finally, it
is believed that in the majority of cases there is not a great difference by using the cannabinoids for cancer pain relief (13).
Advantages of medical cannabis: In the contrary to ∆9-THC, CBD (the second most abundant compound in cannabis) is well tolerated in patients even in relatively high doses. CBD is
also believed to have anti-psychotic, anti-convulsive, anti-inflammatory, anxiolytic and relaxing properties (12). Further, it was observed that the use of an oromucosal spray of
cannabinoids (∆9 -THC: CBD) for a long period, contributed to the reduction of cancer-related pain without increasing the dose in patients. In fact, the particular spray was found
to be efficient to patients resistant to opioids analgesics. Moreover, it was demonstrated that nabilone not only contributed to the nausea, anxiety and pain problem in high staged
cancer people, but also it diminished the use of other drugs including non-steroid anti-inflammatory, anti-emetics, anti-depressing and opioids drugs, comparing to the untreated
with the specific drug patients (14). In addition, during the last decades it has been demonstrated multiple studies, that cannabinoids have antitumor properties in various
cancer cell types including breast tumor, melanoma, pancreatic cancer, brain tumors and lymphomas among others (15).
Conclusion
The outcomes of the conducted studies indicate that nabixomole which constitutes of both THC and CBD, might be an efficient adjunct to cancer pain management in those patients
who are not optimized on opioid treatment. Therefore, medical cannabis might be more beneficial as an adjunct to the standard therapy rather than as a replacement (9).
There is insufficient evidence to conclude that a single low dose morphine equivalent or a single synthetic THC counterpart is more effective in relieving moderate to severe cancer
pain. Moreover, there is low certainty evidence that CBD improves on specialized palliative care alone in terms of reducing pain in patients with advanced cancer (16).
Current studies indicate that there is a potential benefit of the use of the medical cannabis in the cancer-related pain treatment. However, the scale and the amount of the
studies conducted are limited. Further research should be done in this field to establish the use and the efficacy of this promising product in the management of an extremely
common symptom that multiple patient encounter (10). Thus, the guidelines recommend that health care providers should use and educate patients with the already available and
established information. It is highly possible that for some patients, cannabis and cannabinoids might be an arrow in the quiver of their health providers, but until more data
support their use in the cancer treatment, they cannot be widely suggested (9).
More studies need to be conducted in order that medical cannabis can be safely and effectively incorporated into medical treatment plans against cancer in general and caner-related
pain especially (17).
References
1. Häuser W, Welsch P, Klose P, Radbruch L, Fitzcharles MA. Efficacy, tolerability and safety of cannabis-based medicines for cancer pain: A systematic review with meta-analysis of randomised controlled trials. Schmerz. 2019 Oct;33(5):424-436. English. doi: 10.1007/s00482-019-0373-3. PMID: 31073761.
2. Zeng F, Wade A, Harbert K, Patel S, Holley JS, Dehghanpuor CK, Hopwood T, Marino S, Sophocleous A, Idris AI. Classical cannabinoid receptors as target in cancer-induced bone pain: a systematic review, meta-analysis and bioinformatics validation. Sci Rep. 2024 Mar 9;14(1):5782. doi: 10.1038/s41598-024-56220-0. PMID: 38461339; PMCID: PMC10924854.
3. Meng H, Dai T, Hanlon JG, Downar J, Alibhai SMH, Clarke H. Cannabis and cannabinoids in cancer pain management. Curr Opin Support Palliat Care. 2020 Jun;14(2):87-93. doi: 10.1097/SPC.0000000000000493. PMID: 32332209.
4. Green R, Khalil R, Mohapatra SS, Mohapatra S. Role of Cannabidiol for Improvement of the Quality of Life in Cancer Patients: Potential and Challenges. Int J Mol Sci. 2022 Oct 26;23(21):12956. doi: 10.3390/ijms232112956. PMID: 36361743; PMCID: PMC9654506.
5. Boland EG, Bennett MI, Allgar V, Boland JW. Cannabinoids for adult cancer-related pain: systematic review and meta-analysis. BMJ Support Palliat Care. 2020 Mar;10(1):14-24. doi: 10.1136/bmjspcare-2019-002032. Epub 2020 Jan 20. PMID: 31959586.
6. Safi K, Sobieraj J, Błaszkiewicz M, Żyła J, Salata B, Dzierżanowski T. Tetrahydrocannabinol and Cannabidiol for Pain Treatment-An Update on the Evidence. Biomedicines. 2024 Jan 29;12(2):307. doi: 10.3390/biomedicines12020307. PMID: 38397910; PMCID: PMC10886939.
7. Wang L, Hong PJ, May C, Rehman Y, Oparin Y, Hong CJ, Hong BY, AminiLari M, Gallo L, Kaushal A, Craigie S, Couban RJ, Kum E, Shanthanna H, Price I, Upadhye S, Ware MA, Campbell F, Buchbinder R, Agoritsas T, Busse JW. Medical cannabis or cannabinoids for chronic non-cancer and cancer related pain: a systematic review and meta-analysis of randomised clinical trials. BMJ. 2021 Sep 8;374:n1034. doi: 10.1136/bmj.n1034. PMID: 34497047.
8. Breijyeh Z, Jubeh B, Bufo SA, Karaman R, Scrano L. Cannabis: A Toxin-Producing Plant with Potential Therapeutic Uses. Toxins (Basel). 2021 Feb 5;13(2):117. doi: 10.3390/toxins13020117. PMID: 33562446; PMCID: PMC7915118.
9. Sawtelle L, Holle LM. Use of Cannabis and Cannabinoids in Patients With Cancer. Ann Pharmacother. 2021 Jul;55(7):870-890. doi: 10.1177/1060028020965224. Epub 2020 Oct 17. PMID: 33070617.
10. Blake A, Wan BA, Malek L, DeAngelis C, Diaz P, Lao N, Chow E, O’Hearn S. A selective review of medical cannabis in cancer pain management. Ann Palliat Med. 2017 Dec;6(Suppl 2):S215-S222. doi: 10.21037/apm.2017.08.05. Epub 2017 Aug 23. PMID: 28866904.
11. Clarke S, Butcher BE, McLachlan AJ, Henson JD, Rutolo D, Hall S, Vitetta L. Pilot clinical and pharmacokinetic study of Δ9-Tetrahydrocannabinol (THC)/Cannabidiol (CBD) nanoparticle oro-buccal spray in patients with advanced cancer experiencing uncontrolled pain. PLoS One. 2022 Oct 14;17(10):e0270543. doi: 10.1371/journal.pone.0270543. PMID: 36240167; PMCID: PMC9565400.
12. Afrin F, Chi M, Eamens AL, Duchatel RJ, Douglas AM, Schneider J, Gedye C, Woldu AS, Dun MD. Can Hemp Help? Low-THC Cannabis and Non-THC Cannabinoids for the Treatment of Cancer. Cancers (Basel). 2020 Apr 23;12(4):1033. doi: 10.3390/cancers12041033. PMID: 32340151; PMCID: PMC7226605.
13. Hatfield J, Suthar K, Meyer TA, Wong L. The use of cannabinoids in palliating cancer-related symptoms: a narrative review. Proc (Bayl Univ Med Cent). 2024 Feb 8;37(2):288-294. doi: 10.1080/08998280.2023.2301241. PMID: 38343467; PMCID: PMC10857674.
14. Lal S, Shekher A, Puneet, Narula AS, Abrahamse H, Gupta SC. Cannabis and its constituents for cancer: History, biogenesis, chemistry and pharmacological activities. Pharmacol Res. 2021 Jan;163:105302. doi: 10.1016/j.phrs.2020.105302. Epub 2020 Nov 24. PMID: 33246167.
15. Andradas C, Truong A, Byrne J, Endersby R. The Role of Cannabinoids as Anticancer Agents in Pediatric Oncology. Cancers (Basel). 2021 Jan 5;13(1):157. doi: 10.3390/cancers13010157. PMID: 33466435; PMCID: PMC7796497.
16. Häuser W, Welsch P, Radbruch L, Fisher E, Bell RF, Moore RA. Cannabis-based medicines and medical cannabis for adults with cancer pain. Cochrane Database Syst Rev. 2023 Jun 5;6(6):CD014915. doi: 10.1002/14651858.CD014915.pub2. PMID: 37283486; PMCID: PMC10241005
17. Zylla DM, Eklund J, Gilmore G, Gavenda A, Guggisberg J, VazquezBenitez G, Pawloski PA, Arneson T, Richter S, Birnbaum AK, Dahmer S, Tracy M, Dudek A. A randomized trial of medical cannabis in patients with stage IV cancers to assess feasibility, dose requirements, impact on pain and opioid use, safety, and overall patient satisfaction. Support Care Cancer. 2021 Dec;29(12):7471-7478. doi: 10.1007/s00520-021-06301-x. Epub 2021 Jun 4. PMID: 34085149.
Χρησιμοποιούμε cookies για να σας προσφέρουμε την καλύτερη δυνατή εμπειρία στη σελίδα μας. Εάν συνεχίσετε να χρησιμοποιείτε τη σελίδα, θα υποθέσουμε πως είστε ικανοποιημένοι με αυτό..
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.
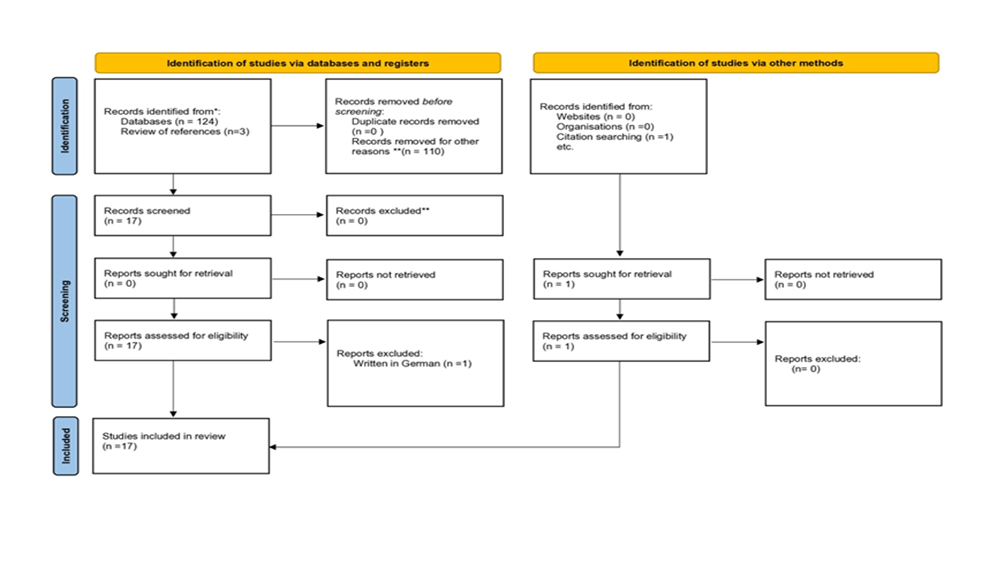 Figure 1: PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources **: title and abstract non relevant
Figure 1: PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources **: title and abstract non relevant